Life, Relationships and Hepatitis B YesYouCan! SA’sWHD Quiz - available in 4 languages hepsa.asn.au/lifeandb
Some photos in this publication may have been altered to disguise identifying details of members of the public.
This resource was prepared and printed on Kaurna Country.
Disclaimer: Views expressed in this newsletter are not necessarily those of Hepatitis SA. Information contained in this newsletter is not intended to take the place of medical advice given by your doctor or specialist.


We welcome contributions from Hepatitis SA members and the general public. SA Health has contributed funds towards this program. ISSN 2651-9011 (Online)

IN THIS ISSUE 1 HR 23 Harm Reduction Conference 4 Hep C Treatment Barriers for Aboriginal People in Remote SA 8 Treating HCV in Children 10 Life, Relationships & Hep B 11 World Hepatitis Day 12 Creating a Home Test for Hep C 13 Prison Health Expo 14 In Our Library 16 Contacts
Correspondence: Please send all correspondence to The Editor at PO Box 782, Kent Town, SA 5071, or email editor@hepatitissa.asn.au
Cover: Cecilia Lim
.
Editor: James Morrison
HR 23 Harm Reduction Conference: Strength In Solidarity
The Harm Reduction conference is held in a different country every 2 years and provides a forum for sharing the latest research, programs and policy in drug use, harm reduction* and human rights. The conference is convened by Harm Reduction International (HRI) – an organisation that promotes harm reduction and rights-based, evidence-based responses to drug use.
What I like about the HRI conference is that HRI always works in partnership with the local Drug User Organisation or peer program to facilitate drug users’ participation in the conference. As the conference was held in Melbourne this year, the local peer-based organisation Harm Reduction Victoria co-hosted the conference.
Awards were given out at the Opening Ceremony, and the inaugural Gill Bradbury
Award (awarded to an individual, group or organisation providing excellent services to people who use drugs) went to the AIVL National Peer Network, of which the Hepatitis SA CNP Peer Projects is a member. It was great to see peers’ contribution to harm reduction acknowledged on an international level. This year the overarching themes were drug law reform (decriminalization of small quantities of drugs for personal use and/or the sale of small quantities of drugs ie ‘user dealers’) and ‘safer supply’, as a result of the tragic impact of fentanyl and its analogues. Fentanyl and fentanyl analogues have contributed to the deaths of many tens of thousands of people in the US and Canada. I can only be thankful that fentanyl has not made huge inroads into the Australian supply but I believe that we must have our SA response prepared if/when it does. The conference presentations and panel discussions were enlightening but it is the opportunities for networking and sharing experiences that I will remember for longer. I was inspired by hearing about civil disobedience and what’s happening on the ground to improve the lives of people who use drugs.
I participated in the workshop to develop the Conference Declaration, which was read out at the closing ceremony. The Melbourne Declaration advocates for the genuine inclusion and representation of people who use drugs, demands equitable health and social outcomes and an end to criminalisation and prohibition of drug use.
HEPATITIS SA COMMUNITY NEWS 98 1
A video of the declaration being read at the closing ceremony can found at youtube. com/watch?v=KkqjCeccUoY
*Harm reduction refers to policies, programmes and practices that aim to minimise the negative health, social and legal impacts associated with drug use, drug policies and drug laws. Harm reduction is grounded in justice and human rights. It focuses on positive change and on working with people without judgement, coercion, discrimination, or requiring that people stop using drugs as a precondition of support (see it at hri.global/what-is-harmreduction).
Carol Holly
This was the first Harm Reduction Conference since 2019 and everyone was excited to hear what Australia had been doing as an early adopter of healthbased approaches to drug use. I wanted to hear about what was going on in the Southeast Asian region, as they are our closest neighbours and notoriously hardline on drug users, with alarming rates of incarceration of women and the use of death penalties for drug offences. Sadly, most of the would-be attendees from Southeast Asia were not given visas.

The conference went for three days: each day we had about 30 presentations to
choose from. It was mindboggling. I would choose something and then question whether I had made the right choice. Most of the presentations I saw were about peers or civil disobedience, focusing on people who had made the choice to do something that was illegal but ethically right. For instance, in Dublin a small organisation had bought a van, which they would park in an alleyway at a certain time of day. This van was an injecting room. Dublin had people injecting and overdosing in the street, so if they could inject safely in a van with a couple of people around them and naloxone on hand, isn’t that a good thing? The police would come and ask them to open up, which they would do after the person had injected the drugs. The police could do nothing as the drugs were gone. Of course, police don’t like this kind of thing and pursued the van with a vengeance. One staff member ended

2 HEPATITIS SA COMMUNITY NEWS 98
up being arrested and charged for not unlocking the van and for obstructing police. He went straight back out the next day. Often their clients were in wheelchairs and needed to be lifted in and out of the van, which was not an easy feat. This van led to changes for injecting drug users in Dublin. The power of people is enormous.
Thinzar Tun from Myanmar’s presentation was called “If there is a will there is a way!—A peer-led Women’s Cost Effective Service Delivery in Rural Areas of Myanmar”. Drug-using women in Myanmar are discriminated against and looked down upon. They struggle to get through each day with no money, no transport and no support from anybody. They paid peer workers to ride motor bikes into rural areas to meet female drug users where they wanted to be met: in shooting galleries, in brothels, and on the street. There they helped them with day-to-day things such as medical appointments and picking up their methadone supplies.
This project helped 194 women in the first year. The cost for each peer, with a bike, was only $37 per year—such a small amount of money to increase women’s quality of life. The only question I had for Thinzar Tun was why did they only employ male peers? Perhaps it had something to do with the
funding, or maybe they were the only drug users they could hire.
Most of the presentations I saw were from countries that have a huge opioid problem, such as Canada, the US and the UK. As drug users are dying by the thousands, the governments and the communities look the other way when people try to do something to ease the pain of all of these deaths, such as having a shop in Canada to sell qualitytested drugs openly to people. As always, effective harm reduction is the only way forward.
Australia is in a different position, as methamphetamine is the favoured drug here. We don’t have massive amounts of opioid deaths, though some people want you to think we do. Sadly, Australia is lagging hopelessly behind and I honestly think people attending the conference might have been disappointed with what we have been doing in the harm reduction and peer space.
I met so many amazing people at this conference, from Canadian drug users to Norwegian nurses. Each and every one of them has a passion for harm reduction and helping the most stigmatised communities in the world. After three days I was exhausted but happy.
HEPATITIS SA COMMUNITY NEWS 98 3
Margie Randle
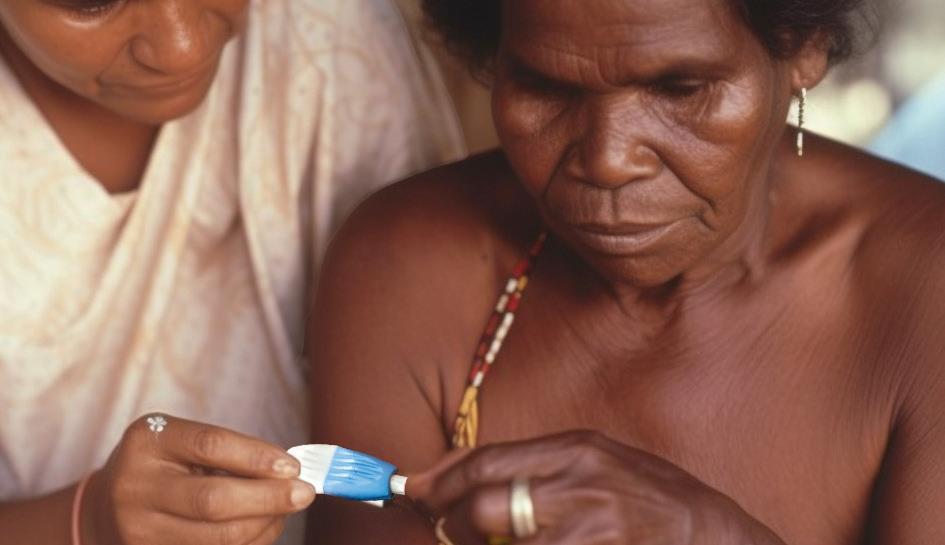
Hep C Treatment Barriers for Aboriginal People in Remote SA
The introduction of direct-acting antiviral (DAA) medications offers the chance to completely eliminate the hepatitis C virus (HCV). Across the world, however, there is a clear disparity in HCV outcomes within Indigenous populations, and in Australia, the rate of infections within Aboriginal and Torres Strait Islander communities is increasing.
Islander Peoples in Rural South Australia: A Service Providers’ Perspective, was published in the International Journal of Environmental Research and Public Health in March 2023.

The study found that key implications for public health policy include emphasising culturally appropriate HCV education for clients, the community, and health service
A new study--believed to be the first published research incorporating a systematic review to explicitly examine the barriers and enablers to diagnosis and treatment amongst rural Indigenous peoples living with HCV in Australia--has looked at what specific problems Indigenous people living in rural South Australia are encountering. The study, Barriers and Facilitators to Hepatitis C Virus (HCV) Treatment for Aboriginal and Torres Strait
providers. Continued efforts to facilitate the uptake of DAA medications for Aboriginal peoples in rural and remote areas should use a multifaceted approach to provide education to clinicians and the community, increasing HCV knowledge and cultural awareness, and aiding in reducing stigma and discrimination.
In Australia, HCV remains one of the most commonly notified diseases, with Aboriginal and Torres Strait Islander peoples
4 HEPATITIS SA COMMUNITY NEWS 98
(particularly in rural and remote areas) recognized as a high-risk population group. Health discrepancies can be exacerbated in rural and remote areas; for example, Aboriginal and Torres Strait Islander peoples living remotely in Australia are 4.3 times more likely to experience a potentially preventable hospitalization than those living in major cities. They are also significantly more likely to be

2013 and 2017, while the rate in the nonIndigenous population decreased by 12%, a concerning statistic in a time of planned global eradication. New HCV infections within the teenage Aboriginal and Torres
diagnosed with HCV, but access to HCV treatment by Aboriginal peoples in remote communities is halved compared to others residing in urban areas.
Worryingly, the most recent data available for Australia as a whole demonstrates that the notification rate for new HCV diagnoses for Aboriginal and Torres Strait Islander peoples increased by 15% between

Strait Islander male population (aged 15–19) were nine times higher than rates in the non-Indigenous population in the same age group.
Most health service providers interviewed as part of the study identified that both
HEPATITIS SA COMMUNITY NEWS 98 5
behavioural risk factors and limited knowledge regarding HCV transmission could mean that people are unaware they are at risk of HCV, while one indicated that people would be aware of HCV and some risk factors, such as intravenous drug use, but might not be aware of other modes of transmission. All agreed that there was limited knowledge of the new DAA medications for Aboriginal peoples at risk of HCV, and that therefore their clients might not know that HCV is curable. There was also hesitancy to adopt the new DAAs due to personal or community experience of the much more severe side effects and lower efficacy of previous interferon-based therapies.
Furthermore, study participants suggested that lower levels of education and poorer engagement with health services were barriers to HCV treatment within regional and remote Aboriginal communities. Health services were the locations where clients were most likely to notice information about DAAs, so poor engagement with these services could contribute to the lack of knowledge in the rural community.
In interviews with residents of regional and remote Aboriginal communities, many people pointed out that cultural obligations could delay treatment uptake and contribute to poor medication adherence and loss of follow-up. Healthcare workers confirmed these obligations might take precedence over a person’s health: responsibilities in looking after an extended family or the increased burden of dealing with the illnesses of loved ones, and being involved in a high number of funerals. “Sorry business” in Aboriginal communities was more important for clients to attend and a
higher priority than health appointments. Study participants suggested that a counterintuitive delaying of treatment until social and emotional needs have been met could contribute to improved outcomes.
The asymptomatic nature of early HCV infection may impact treatment uptake and completion in rural Aboriginal communities, as clients often do not feel acutely unwell for many years. However, study participants also highlighted that HCV could be considered less of a priority when other comorbidities and Aboriginal peoples’ social and emotional

6 HEPATITIS SA COMMUNITY NEWS 98
wellbeing are also affected. Over time, the accumulative nature of problems can become overwhelming. Therefore, an approach that focuses on holistic healthcare, which supports both emotional and spiritual health as well as physical, could result in better engagement in health services within regional and remote communities.
Interviews about barriers to accessing treatment emphasised the typically long wait times for referrals to clinicians with HCV treatment knowledge and experience. A shorter wait time between diagnosis and appointments could help reduce the distress associated with being diagnosed. Not linking clients to services or not having frequent and regular specialist access was also identified as a barrier to HCV treatment in a rural setting. Telehealth services within Indigenous communities can help overcome these barriers.
For some, the transient nature of living was noted as a complicating factor that must be considered: frequent moving from place to place was mentioned by study participants as a primary reason for the disruption to the continuity of care and poor medication adherence. However, participants felt that point-of-care (POC) testing had been very beneficial within regional and remote Aboriginal communities, particularly with transient clients. One focus group also spoke about their relationship with the local prison in providing health summaries after discharge, which enabled follow-up with their clients, further illustrating the benefit of cross-provider solid relationships where strong rapport is built.
‘Transient’ healthcare workers in regional and remote areas was also noted as a problem:
some services indicated they relied on locum doctors, and felt this did not allow clients to build sufficient rapport with their clinicians. This jeopardized the aim of providing holistic care, as clients were less likely to discuss their HCV risks, diagnosis, or treatment without trust.
Finally, the related issues of confidentiality, stigma, discrimination, and shame were seen as key issues. Many clients reported concerns regarding how others would perceive them if they disclosed their HCV status, while many also reported previous general negative experiences as Indigenous people within mainstream health services encountering discriminatory attitudes and treatment. Cultural shame was also reported as an important problem: clients often believed they would bring shame to themselves and their friends and family through their HCV status and, consequently, be alienated by their communities. This greatly impacted clients’ cultural identity, with some describing it as the ‘broken spirit’ disease.
Overall, the study emphasises the importance of culturally appropriate HCV education for clients, the community, and health service providers. Continued efforts to facilitate the uptake of DAA medications for Aboriginal peoples in rural and remote areas should use a multifaceted approach to provide education to clinicians and the community, increasing HCV knowledge and cultural awareness, and aiding in reducing stigma and discrimination.
READ MORE:
ncbi.nlm.nih.gov/pmc/articles/ PMC10002019
HEPATITIS SA COMMUNITY NEWS 98 7
Act Now! Treating HCV in Children is Safe and Effective
There are 3.5 million children around the world living with chronic hepatitis C. In Australia, the prevalence is estimated to be at least 0.4 cases per 100 000 children under the age of 15 years. Chronic hepatitis C in children can often move very slowly, but it may still progress to hepatic fibrosis, chronic liver disease, and hepatocellular cancer. These often marginalised children experience reduced quality of life, social stigmatisation, and inadequate access to specialist care. Research led by Jessica Eldredge and published in the Medical
Journal of Australia argues that early treatment of HCV in children is cost-effective and reduces the lifetime impact of chronic liver disease and its side-effects. The study, Direct-acting antiviral treatments in Australia for children with chronic hepatitis C virus infection, was published in January.
Australia-wide, direct-acting antiviral (DAA) treatments have revolutionised the management of HCV infection since they were made available on the Pharmaceutical Benefits Scheme in 2016. In 2020 age restrictions for several DAAs were removed.

Dr Eldredge’s team examined outcomes for children under 18 years of age with HCV infection treated with DAAs in the four years between April 2018 and April 2022 at five tertiary children’s hospitals across three Australian states. Fifty-four children with HCV infection commenced DAA treatment at the five participating hospitals during the study period, using four different DAA combinations. Nine of these patients were Aboriginal or Torres Strait Islander people. None of the children had received previous treatments for HCV infection. None had documented cirrhosis, but liver biopsy identified early fibrosis in one child. Four of the children had foetal alcohol spectrum disorder. Perinatal viral transmission was suspected in 51 of the cases, while injecting drug use was known to be the source of infection in the other three.
Over the course of the study, two children could not be followed up, and one did not complete treatment because of difficulty swallowing the DAA tablet. Fifty of the fiftyone children who completed treatment and were followed up had no detectable HCV in their bodies 12 weeks after treatment, and, like the child who did not complete the treatment, the fifty-first had also had trouble swallowing the tablets, leading to erratic adherance.
The DAA treatments were well tolerated, and the results show that they were highly effective at treating HCV infections in children, which is consistent with their efficacy in children and adolescents in
clinical trials worldwide. Adherence to therapy was shown to be important when treating younger children; making use of smaller tablets or powdered medication was also shown to be of use for those children who have trouble swallowing standard-sized pills, and improved treatment efficacy for them as well.
The World Health Organization has set the ambitious target of eradicating HCV globally by 2030. It has recently been projected that only 72% of Australians (all ages) with chronic HCV infection will be treated by that year. Screening infants and children at particular risk should be the priority, with a focus on early referral to tertiary specialists with experience in treating HCV infection in children. Treating infected Australians early in life will minimise the risk of them being lost to medical follow-up, as well as reducing liver-related morbidity, social stigmatisation, and the risks of vertical and horizontal viral transmission.
READ MORE:
onlinelibrary.wiley.com/doi/full/10.5694/ mja2.51852
hepcguidelines.org.au/wp-content/ uploads/2021/11/HCV_in_Children_ Guidance_Final_Nov2021.pdf
onlinelibrary.wiley.com/doi/10.1111/ jpc.12904
HEPATITIS SA COMMUNITY NEWS 98 9
Life, Relationships and Hepatitis B
“Hello…hello,” the woman called to me. “Do you work there?” she asked pointing to the Hepatitis SA office. I nodded.
“Can I talk to you, ask you something?” she continued. She needed to get back to the hospital where she worked; her lunch break was almost over, so we spoke as she walked. She told her story and gave me her contact details.
Her nephew had just got engaged and wasn’t sure if he should tell his fiancé’s family about his positive hepatitis B status. She was worried that the family, if they knew, would oppose the relationship.

with proper management, it is possible to minimise the impact of the virus and live a normal life. The two key tools are:
Regular monitoring: see a doctor at least once every six months for a liver check and blood tests.
Vaccination: get family and household members tested for hepatitis B.
Monitoring
Although there is currently no cure for hepatitis B, there is treatment to manage the virus. While not everyone with hepatitis B needs treatment, six-monthly liver checks and blood tests will ensure that treatment can be given without delay, if and when it is needed.
Vaccination
The easiest and best way to protect people close to you is a safe and highly effective vaccine available to people of all ages. For most people three doses over six months will provide life-long protection.
She was looking for a hepatitis B-friendly doctor who spoke their language, a GP her nephew could consult, and his fiancé’s family could talk to.
In communities from regions of higher hepatitis B prevalence, such stories are not unusual. The adverse outcomes of chronic hepatitis B would be familiar, and the fear of transmission – particularly to children –would be real, especially where childhood hepatitis B vaccination is not universal.
For some, a hepatitis B diagnosis must seem like a huge barrier to a normal life. What many don’t realise is that in Australia,
If immunity does not develop after three doses, extra doses may be needed. Your family and household could be eligible for free hepatitis B vaccinations. (https://bit.ly/ hepbvax-eligibility-sahealth.)
Pregnancy
Hepatitis B is transmitted via blood and sexual fluids; babies do not inherit hepatitis B through their parents’ genes.
Hepatitis B may be passed to a baby during their birth, but this can be prevented with a dose of vaccine and immunoglobulin given to baby in the first four to twelve hours after birth. Immunoglobulin is a blood product with hepatitis B antibodies. If needed, treatment of hepatitis B may be given during pregnancy to
10 HEPATITIS SA COMMUNITY NEWS 98
reduce transmission risk to the baby. A person living with hepatitis B can safely breastfeed their baby, unless there is bleeding from the nipples..
Staying healthy

In addition to regular monitoring, a healthy diet and keeping as physically active as possible will help maintain liver health. Also important is limiting fat and alcohol intake as these are damaging to your liver.
If you are not immune to hepatitis A, get a vaccination aganst it as well, as any additional liver infection would put further strain on your liver.
Conclusion

With proper care, hepatitis B should not stop you from living a full, healthy life with your family.

And in case you’re wondering, we found a friendly GP who spoke that family’s language. Although his books were closed, he made an exception and agreed to see them.
Cecilia Lim
Our quiz on LiFe aNd HePatitis B launches on World Hepatitis Day, 28 July.

HEPATITIS SA COMMUNITY NEWS 98 11
All
Look out for it. Have a go!
entries will go in the Draw for a $500 Visa Giftcard.
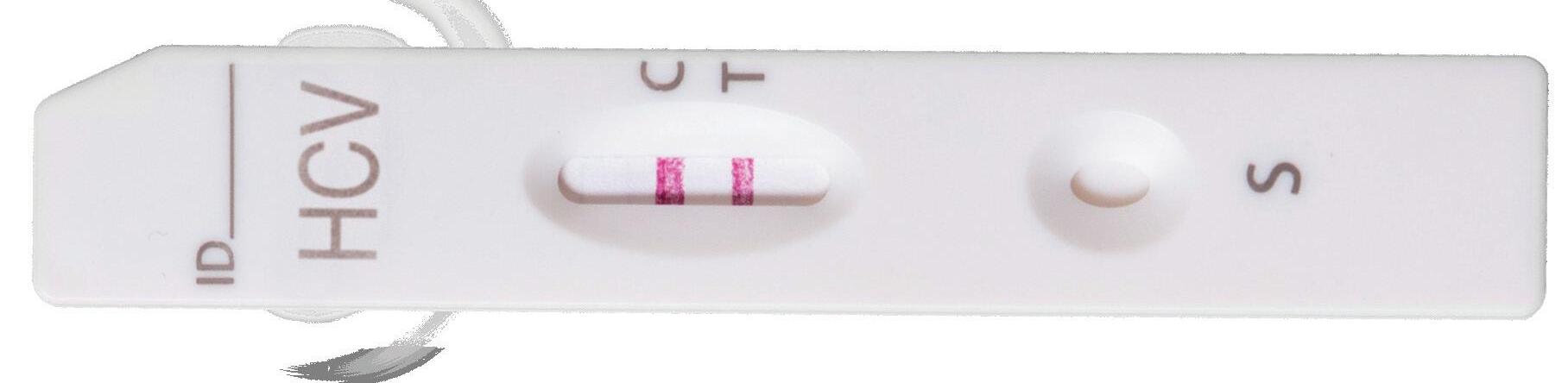
Creating a Home Test for Hep C—with AI
Going beyond pregnancy and COVID-19, the world could someday soon come to rely on at-home tests for many diseases thanks in part to “artificial intelligence”. University of Florida scientists have used artificial intelligence tools to simplify a test that works for both hepatitis C and SARS-CoV-2, the virus that causes COVID-19. The simplified test happens in one small test tube in just a few minutes. With further refinement, it could come to doctor’s offices soon and, one day, even home tests that are as easy as a pregnancy test.

“We are trying to build a home-based test that is as reliable as a lab-based test,” said Piyush Jain, who led the latest research. His group is working on a system known as a one-pot reaction, because the entire test happens in one small test tube. These tests, based on a technology known as RTLAMP, can amplify small portions of a virus’s genome and produce a visible signal when it detects the virus. Reading these tests can be as simple as looking for a blue colour or using a small device that detects a change in the test tube, the sort of thing many readers will be familiar with from doing home rapid antigen tests (RATs) for COVID-19.
However, many RATs have a relatively high false positive rate, meaning they aren’t as reliable as they could be, so Professor Jain’s team are adding another technology, called CRISPR, to determine the difference between a false positive and a true positive.
CRISPR is a very precise genetic engineeing tool. Jain’s group relies on the CRISPR
system’s ability to home in on particular genetic sequences. This means that only if the sequence for, say, the hepatitis virus is really present will the test show a positive result.
However, the RT-LAMP technology requires a temperature of 65°C, while CRISPR works best at human body temperature. That difference makes tests far more complicated when they require two separate reactions— too complicated for at-home use. Jain’s team has been trying to bridge this gap by developing a CRISPR system that can withstand higher temperatures.
From a heat-loving species of bacteria, the researchers recently discovered a CRISPR enzyme that thrives at around 60°C, almost high enough. Jain’s group turned to AI tools to analyse this enzyme and discover how they could make it survive at 65°C. The AI programs suggested a few dozen changes to the enzyme, which Jain’s group tested in the lab. They eventually found four changes to the enzyme that successfully changed it to work at the ideal temperature.
“It’s very challenging for any human to do this kind of analysis on an enzyme. We didn’t have to spend years, we could make these improvements in months,” Jain said. “With everything working at the same temperature, now we are able to combine everything in a true one-pot reaction, which we call SPLENDID.”
The team verified their simplified SPLENDID test on clinical samples from patients with hepatitis C or COVID-19. The test was
12 HEPATITIS SA COMMUNITY NEWS 98 Illustration by Freepik
97% accurate for SARS-CoV-2 and 95% accurate for the most prevalent version of the hepatitis C virus found globally. Although it didn’t work well against other strains of HCV, straightforward changes to the test should quickly improve its accuracy, Jain says. Once
this is done, he hopes to verify it in hospital settings in hopes of one day providing athome tests as well.
READ MORE:
Read the study at bit.ly/splendid_research
Quizzing and Testing at Prison Health Expo
It was a busy day in the Mobilong gym on 17 May as its first Prison Health Expo for the year got underway.
Hepatitis SA workers received 288 quiz entries, carried out 22 Hepatitis C Point of Care tests (HCV PoCT) and registered another 39 prisoners who were keen to get tested.

“We ran out of time to process the tests for everyone who expressed interest,” said Hepatitis SA Information and Support Coordinator, Lisa Carter. “We are now liaising with SA Prison Health Service to provide testing for those who missed out on the day.
“This can be us going in again to do testing at the health centre or SA Prison Health providing conventional needle and syringe testing.”
Hepatitis SA Education Coordinator, Jen Grant, said there was a good range of services offering information and activities at the Expo. “The Cancer Council was there with
a machine that checks for skin damage, and nurses from Mobilong’s health centre offered blood pressure checks and liver scans with fibroscan machines provided by the RAH,” said Jen.
Hepatitis SA’s quiz included two simple questions on hepatitis B and C treatments and two practical prizes (a pair of socks and a packet of Tim-Tams) for each group of participants.
Other services present included AA, Aboriginal Services, and Mosaic counselling service.
HEPATITIS SA COMMUNITY NEWS 98 13
With international Men’s Health Week in June, we focus on some of the issues that influence how men maintain their health in general, and liver health in particular. Almost 1 in 5 men in Australia wait longer than they feel is acceptable before getting an appointment with a GP*, and men often use drugs or alcohol to deal with health issues and stress. Men in Australia are three times more likely to be diagnosed with liver cancer than women**. Difficulties with help seeking behaviour, dealing with stress, drug and alcohol use, as well as maintaining sexual health can all seriously impact men’s health and wellbeing. The following resources aim to inform and support practitioners and men in the community to address these issues. All are free to access online.
* AIHW, The health of Australia’s males, Canberra, 2019 bit.ly/ausmalehealth
** Aust. Govt. Cancer Australia, Liver cancer in Australia statistics, Canberra, 2022 bit.ly/livercancerstats
In Our Library

Men’s Health and Liver Disease
Men’s Health Information and Resource Centre: publications Western Sydney University, Sydney. Website. Practitioner guides to accessible health care for men, effective men’s health messaging, men and mental health plus other evidence based publications about men’s health. bit.ly/mensinfo_resources


Mensline – help with addiction
Mensline Australia, Melbourne. Articles and online/video chat line.
Articles about how to recognise and seek help with addiction (drugs and alcohol) and its impact on physical and mental health - with access to phone, online and video counselling. bit.ly/mensline_addiction

Health behaviours of Australian men and the likelihood of attending a dedicated men’s health service

BMC Public Health, Bethesda, 2018. 10p.
70% of men reported a moderate or higher likelihood of attending a DMHS. Redesigning primary health services may enhance timely and effective uptake by men. bit.ly/menshealthservice
Men’s business
Our Mob and Cancer, Sydney. Webpage and video. Discusses the importance of culture and how men can conduct men’s business, upholding or supporting roles and responsibilities particularly during a cancer journey.
bit.ly/mensbusiness_cancer
14 HEPATITIS SA COMMUNITY NEWS 98
Know your man facts: toolkits for talks and sharing

Australian Men’s Health Forum, Sydney. Website.
Toolkit of resources to use in groups, the workplace or at community events. Includes notes, posters and social media tiles for mental health, mateship, and common health risks.

bit.ly/manfacts
Hepatitis B


Gay Men’s Health Australia, Melbourne, 2015. 16p article; 1 minute video
Gay friendly doctor, George Forgan-Smith, outlines the transmission risks, symptoms, tests and treatment for hep B. bit.ly/hepb_gaymen
What to know about hepatitis C in men

Medical News Today, Bexhill-onSea, 2023. 8p article
Hepatitis C virus appears to affect males more often than females: this article talks about the main symptoms for men, risk factors, testing, treatment and prevention.
bit.ly/men_hepc
To see a listing of all available resources on this topic, visit bit.ly/librarymen.
Find a service – HIV and STI testing
Emen8, Australia. Website. Sexual health and wellbeing initiative for gay, bisexual and other men who have sex with men: search engine for STI testing sites including those run by peers.
bit.ly/emen8testing
HEPATITIS SA COMMUNITY NEWS 98 15
Photo by Senivpetro/Freepik
Hepatitis sa provides free information and education on viral hepatitis, and support to people living with viral hepatitis.
Postal Address: Kaurna Country PO Box 782
Kent Town 5071
(08) 8362 8443



1800 437 222
www.hepsa.asn.au
HepSAY Blog: hepsa.asn.au/blog
Library: hepsa.asn.au/library
@HepatitisSA
@hep_sa
Resources: issuu.com/hepccsa

Email: admin@hepatitissa.asn.au
HEPATITIS SA BOARD



Chair

Arieta Papadelos
Vice Chair
Bill Gaston Secretary
Sharon Eves
Treasurer
Michael Larkin
Ordinary Members
Catherine Ferguson
Bernie McGinnes
Sam Raven
Joshua Riessen
Salma Safi
Kerry Paterson (CEO)
Free hepatitis A, B and C information, confidential and non-judgemental support, referrals and printed resources.
We can help. Talk to us. Call or web chat 9am–5pm, Mon–Fri
Information Support

1800 437 222
hepsa.asn.au

Hepatitis SA has a wide range of hepatitis B and hepatitis C publications which are distributed free of charge to anyone in South Australia.
To browse our collection and place your orders, go to hepsa.asn.au/orders or scan the QR code below:

16 HEPATITIS SA COMMUNITY NEWS 98
Because it is the only one you have and you can’t How Do I Love My Liver? Pr and alcohol. egular ex educe alcohol intak standar oid binge drinking don’ Why Love My Liver? Why Love My Liver? or hepatitis and B to find out more. Hepatitis Hepatitis SA provides information, support and education to people affected by hepatitis, and health and community work Because it is the only one you have and you can’t live without it! How Do I Love My Liver? er against main Why Love My Liver? Why Love Liver? Get accinated or hepatitis and tooing and other pr equipment not to find out more. 3 y g 1300 437 222 Hepatitis SA provides information, support and education to people affected by hepatitis, and health and community work you have and you can’t live without it! How Do I Love My Liver? Why Love My Liver? Why My Liver? tooing and other pr y g 1300 437 222 p Hepatitis SA provides information, support and Keeping up your exercise regime can sometimes be Don’t let yourself get bored—try different Promise yourself healthy rewards (perhaps Exercise with partner or group. Having 437 222 or visit Hepatitis SA online at hepatitissa.asn. explore the catalogue online at hepsa.asn.au/library health.gov.au/internet/main/publishing.nsf/content/healthartwork Hana Jang, used under Creative Commons license: [flickr.com/photos/from_drawing] Exercise for Healthy Livers SAHealthhascontributedfundstowardsthisProgram. Once you’re comfortable with this, you can too hard, you might end up feeling overtired or run-down, which can make you more likely altogether and undo all the work things off, but then you run the risk of giving (perhaps high-quality healthy treats, or harder for you to drop out, and you can that it becomes a normal part of your Hepatitis SA has lots of useful information Visit our library online at hepsa.asn.au/ the Australian National Physical Activity The Heart Foundation has number of helpful Exercise for Healthy Livers Hepatitis SA towards this Program. Fibroscan What is it, and how will it help me? Hepatitis SA www.hepatitissa.asn.au What are the risks? fibroscan. Fibroscan scores are very useful tool, but they are not the whole picture. Your doctor or nurse will take into account all the information they have about your health when they make recommendations to you about your treatment options, not just the scan results. how isapplied 1800 437 222 hepsa.asn.au Support Living with Advanced Liver Disease Helpful Hints § Gum Infections Infected gums bleed when brushed, or may swell or redden. Receding gums, loose teeth and bad breath are also symptoms of gum infection. Decay, above) Using interferon (occasionally used as treatment for hepatitis C) or smoking can lower your resistance to gum disease holding the brush at 45° to the gum line and moving the brush in small circles Use dental floss on the gaps between teeth and on the surfaces of teeth Use an antibacterial mouthwash, preferably alcohol-free (like PerioGard) Denture Care each meal, and clean them daily with a soft brush and mild soap. Don’t use toothpaste, as this will wear the dentures away. Dentures should be removed at night and left to soak in cold water while not in Warning People with cirrhosis or blood/ bleeding disorders, or who are taking interferon, should talk to dentist about any special precautions which may be Hepatitis C & Dental Care C Cartoon The Divine Harvester Hepatitis SA (08) 8362 8443 Kaurna Country Hepatitis C Treatment There are highly effective cures for hepatitis or no side effects. These drugs, known as direct acting antivirals, are available on the Pharmaceutical Benefits Scheme (PBS). Hepatitis C Information for Family & Friends
Viral Hepatitis Community Nurses
Viral Hepatitis Nurses are nurse consultants who work with patients in the community, general practice or hospital setting. They provide a link between public hospital specialist services and general practice, and give specialised support to general practitioners (GPs) to assist in the management of patients with hepatitis B or hepatitis C. With advanced knowledge and skills in testing, management, and treatment of viral hepatitis, they assist with the management of patients on antiviral medications and work in shared care arrangements with GPs who are experienced in prescribing medications for hepatitis C or accredited to prescribe section 100 medications for hepatitis B. They can be contacted directly by patients or their GPs:
CENTRAL: QUEEN ELIZABETH HOSPITAL
Jeff: 0423 782 415
Amanda: 0466 851 759
Debbie: 0401 717 953
NORTH
Bin: 0401 717 971
Serena: 0413 285 476
Specialist Treatment Clinics
SOUTH
Rosalie: 0466 777 876
Lucy: 0466 777 873
OFFICE: (08) 8204 6324
Subsidised treatment for hepatitis B and C are provided by specialists at the major hospitals. You will need a referral from your GP. However, you can call the hospitals and speak to the nurses to get information about treatment and what you need for your referral.
• Flinders Medical Centre Gastroenterology & Hepatology Unit: call 8204 6324
• Queen Elizabeth Hospital: call 8222 6000 and ask to speak a viral hepatitis nurse
• Royal Adelaide Hospital Viral Hepatitis Unit: call Anton on 0401 125 361
• Lyell McEwin Hospital: call Bin on 0401 717 971
Don’t like Talking? No Problem.
Visit hepsa.asn.au - no need to log in, lots of info & pdates
Follo the HepSAY blog - hepsa.asn.a /blog
Order print resources - hepsa.asn.a /orders/
Follo s on T i er @hep_sa or Facebook @Hepa sSA
ALL ser ices & reso rces FREE

2 HEPATITIS SA COMMUNITY NEWS 98 • • • • Do you work with community members at higher risk of hepatitis B? Celebrate World Hepatitis Day with us!