#97 • April 2023 Community News FREE! Please take one Prisons: The Weakest Link in the Fight Against Hepatitis Plus Safe Breastfeeding and more
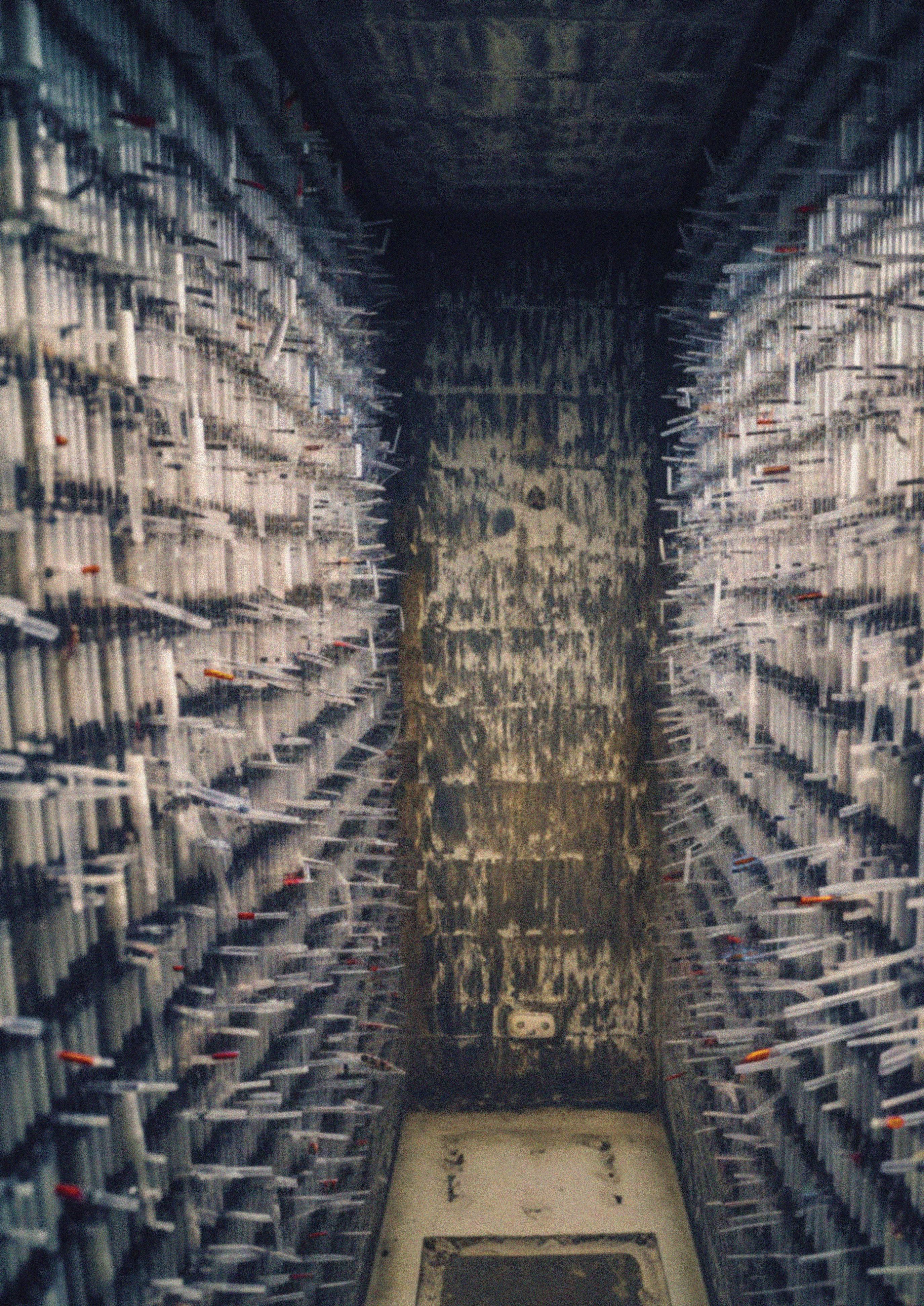
Cover: The lack of clean injecting equipment helps make prisons the weakest link in the fight against blood-borne viruses like hepatitis B and C—see p10. Image by James Morrison. Correspondence: Please send all correspondence to The Editor at PO Box 782, Kent Town, SA 5071, or email editor@hepatitissa.asn.au.

Editor: James Morrison
Some photos in this publication may have been altered to disguise identifying details of members of the public.
This resource was prepared and printed on Kaurna Country.


Disclaimer: Views expressed in this newsletter are not necessarily those of Hepatitis SA. Information contained in this newsletter is not intended to take the place of medical advice given by your doctor or specialist.

We welcome contributions from Hepatitis SA members and the general public. SA Health has contributed funds towards this program.
ISSN 2651-9011 (Online)
IN THIS ISSUE 1 Improving Liver Cancer Detection 2 Mother-Baby HBV Transmission 3 Breastfeeding is Safe with Hep B 4 Health Expos 6 POC Testing 10 Prisons: The Weakest Link 12 10 Strategies for Prisons 14 In Our Library 16 Contacts
More Evidence of DAAs’ Power for Elimination
A recent large-scale study confirms that treating chronic hepatitis C patients with direct-acting antivirals (DAA) leads to improved outcomes and better long-term survival.
The study, published in JAMA Internal Medicine, used data from a large database of over 60 million people across the US, and included over 245,000 adults with chronic hepatitis C.
The study compared two groups of patients: those who were treated with DAAs and those who were not. The results showed that the treated group had a significantly lower chance of developing serious liver problems, including hepatocellular carcinoma, as well as other health issues less commonly thought of as being directly linked to
hepatitis C, like diabetes, chronic kidney disease, cardiovascular disease, and nonhepatic cancer.
The study also found that the treated group had a lower rate of death.
The researchers believe that these results support the idea that all patients with hepatitis C should receive DAA treatment, regardless of their financial situation or how far the disease has progressed, something which is a central part of Australia’s National Hepatitis C Strategy.
READ MORE:
jamanetwork.com/journals/ jamainternalmedicine/articleabstract/2799370
HEPATITIS SA COMMUNITY NEWS 97 1
Ending Mother-Baby Hep B Transmission

Mother-to-child transmission of hepatitis B occurs frequently either in the uterus, through placental leakage, or through exposure to blood or blood-contaminated fluids at or around the time of birth. This form of transmission (sometimes called “vertical transmission”) is believed to account for between a third and a half of hepatitis B infections, and so a way to easily prevent it would do a huge amount to reduce the number of people living with hepatitis B in the long term.
Early results from a randomised Chinese clinical trial have shown a possible way to make this happen. Using the medication known as maternal tenofovir disoproxil fumarate (TDF) in combination with infant vaccination against hepatitis B completely eliminated vertical transmission of the hepatitis B virus. This was the case even when the mothers had extremely high loads of hepatitis B virus in their blood.
Another exciting aspect to this trial is that there was no need to use hepatitis B immunoglobulin, something which is often used to give people a temporary immunity
against hepatitis B in high-risk situations, or immediately after exposure as a form of prophylaxis. Supply of this immunoglobulin is often very limited, and so anything which reduces demand is extremely helpful.
The mothers themselves also showed dramatically lowered levels of hepatitis B in their blood at the time of birth, and there was no increase in the risk of congenital defects.
Dr Calvin Pan told an audience at The Liver Meeting, one of North America’s largest hepatology conferences, that the findings showed that use of this t2o-part treatment “could effectively prevent transmission, which is comparable to the current standard of care, with no safety signals.”
This sort of 100% success rate is extraordinarily rare in medical trials, and so further larger trials are now needed to confirm and extend these results.
READ MORE:
clinicaltrials.gov/ct2/show/NCT03476083 medpagetoday.com/meetingcoverage/ aasld/101644
Breastfeeding is Safe with Hepatitis
You can breastfeed safely with hepatitis B or hepatitis C.
There is a common misconception that people living with hepatitis B and/or hepatitis C cannot safely breastfeed. Recent misleading media coverage published by News Limited has suggested that drinking breast milk can easily pass on hepatitis B and hepatitis C. This is not the case.
It is safe to breastfeed if you have hepatitis B.
If you have hepatitis B, your baby should get two injections the day they are born.
If you have hepatitis B, your baby has these injections within the first 12 hours. One injection contains immunoglobulin. These are antibodies that help the body fight the virus. The second injection is baby’s first regular hepatitis B vaccine. All babies get this vaccine, even if their mother doesn’t have hepatitis B. They’ll also get regular hepatitis B vaccines over the next 6 months.
Once your baby has received their immunoglobulin injection it is safe to breastfeed.

It is safe to breastfeed if you have hepatitis C.
Breastfeeding does not spread hepatitis C. Your baby cannot get hepatitis C from your breast milk. You should stop breastfeeding if you have cracked and bleeding nipples. This is because hepatitis C spreads by infected blood. If this happens to you, talk to a midwife or GP. It’s a good idea to breastfeed whether or not you have hepatitis C.
There is a cure for hepatitis C. In most cases it only requires 8-12 weeks of tablets. Hepatitis C cures should not be taken when pregnant.
READ MORE: bit.ly/pregbirthbeyond issuu.com/hepccsa/docs/mums_to_b_ brochure
HEPATITIS SA COMMUNITY NEWS 97 3
Health Expos

Hepatitis SA has been fortunate enough to attend community health expos for many years and are delighted that these events have come back after a short hiatus due to COVID. In February and March this year, Hepatitis SA attended the Australian Refugee Association Health Expo in Salisbury and the Sonder Close the Gap Event at Wayville Showgrounds.
The Australian Refugee Association (ARA) Event was held on Thursday, 23 February at the Salisbury Community Hub. Eighteen services were in attendance, providing information and education to the community. The Education team from Hepatitis SA attended and engaged with people from multiple different communities including Afghani, Venezuelan, Syrian, Filipino, and Spanish.
A total of 28 people from the event entered our quiz raffle to win a voucher. We used this quiz to talk to community members to ensure they had a solid understanding of hepatitis C treatment and hepatitis B monitoring.

The Sonder Close the Gap Day event was held in the Jubilee Pavillion at Wayville Showgrounds on Thursday, 16 March. This event is held each year, and jointly presented by Sonder (who provide services to support mental health, alcohol and other drug use, homelessness, disability, employment, Aboriginal health and chronic disease) and Nunkuwarrin Yunti (who provide contemporary, culturally based health, social and emotional wellbeing services to build a healthy Aboriginal and Torres Strait Islander community). Both Hepatitis SA’s education team and the Clean Needle Program Peer Project team attended the event.
The education team engaged a henna artist to provide free henna to attendees as an example of safe body art. While attendees were lining up for the henna, it was an excellent opportunity for staff to chat with them about viral hepatitis.
The event was opened with a Welcome to Country by local elder Uncle Moogy, and had many musical acts performing throughout the day including Katie Aspel, the Tal-Kin-Jeri Dance Group, Nathan May, the Nancy Bates Trio and Eddie Peters. It was attended by many health and community services who were there to provide information to attendees, as well as various health checks. There were also many fun activities to participate in like jumping castles, kids craft, Jiu Jitsu demonstrations, live music, an animal farm as well as a meet-and-greet with some AFL and SANFL players. There were well over 1000 people who attended the event, and the educators engaged with 87 community members for the quiz raffle.



World-first Hep C Point-of-Care Testing Program
South Australian Viral Hepatitis Nurses are joining a world-first HCV point-of-care testing program being rolled out nationally in Australia. This follows community campaigns last year that brought hepatitis C rapid testing to the Riverland and Port Pirie.
Murray Bridge – the site of Hepatitis SA’s first LiverBetterLife project in 2017 – is one of the rural sites for the National Australia HCV Point of Care Testing Program’s initiative in South Australia.
Viral Hepatitis Nurses Rosalie Altus and Lucy Ralton from the Southern Adelaide Local Health Network (SALHN) together with Hepatitis SA have connected with local services to plan regular point of care testing sessions in the regional city, beginning in March.
Why Murray Bridge?
“Murray Bridge is an area with a lower socio-economic index that’s been deeply affected by drug use in recent years,” said Lucy. “Compared to Greater Adelaide, it has a higher proportion of unemployment and people looking for work as well as people with a disability.

“These are all factors associated with a higher risk of hepatitis C infection.”
Hepatitis SA educators will provide a series of free education sessions to workers in mental health care, community corrections, drug and alcohol services, and other community services, as well as GP networks. The sessions will cover basic hepatitis C information, risk factors, diagnosis and
treatment, and also inform the workforce about the national point-of-care testing program and its roll out in Murray Bridge. Rosalie and Lucy will coordinate with services which express interest in hosting the point-of-care testing clinics for their clients and work out the best time and format for each clinic location.
Because it takes a bit of time for new projects to build up momentum and for relationships with key local people and services to develop, the nurses will trial regular testing clinics for six months to see what the uptake is like.
“We’ll adapt the where, when and how as we go so that we can optimise the opportunity to bring hepatitis C point of care testing to people in the Murray Bridge area,” said Lucy.
ACCHO Clinics
In addition to community clinics run by the viral hepatitis nurses, there will be hepatitis C point-of-care testing clinics at the Moorundi Aboriginal Controlled Health Service in Murray Bridge and Pangula Mannamurna in Mount Gambier, both of which are also registered HCVPOCT sites.
According to HCVPOCT Project Coordinator, David Silk, rural sites make up around 25% of total testing sites. Murray Bridge together with Moorundi and Pangula Mannamurna will form the core of South Australia’s rural testing sites.
Moorundi’s Aboriginal Health Clinical Director, Beth Hummerston, said hepatitis C point of care testing will work well at their
clinics, particularly in Murray Bridge as they will soon become a Clean Needle Program (CNP) site.

“Community feedback was that the current options available to access clean needles are not places where people feel comfortable going,” she said.
“Having a CNP available may provide opportunities to talk to people about hepatitis C testing and is a way of addressing disparities in health services for people who likely don’t access health services regularly.”
She said testing could be provided on a day to day basis as need and opportunity arise, or there could be clinic days where people are encouraged to turn up for pointof-care testing. “It depends on community response,” she said.
“We have very experienced Aboriginal Health Practitioners who can perform the testing services independently, so we would be able to offer point of care testing opportunistically, in response to circumstances. We can be flexible.”
She said Moorundi hopes to eventually take the point of care machine to other communities where they have clinics at Raukkan and Victor Harbor.

Treatment and Follow-up
Hepatitis C treatment is just a matter of taking tablets daily for eight or twelve weeks. Close to 100% are cured with retreatment options available to the very small percentage of people for whom treatment did not work the first time.
“For people who test positive, we can book them with our GPs. This will ensure the experience is culturally comfortable and nonintimidating,” Beth said.
Similarly, those who test positive at the clinics run by the viral hepatitis nurses can be immediately referred on for treatment to be managed by their GPs. For those who don’t have a GP, alternative arrangements can be made.
“People in rural and regional areas often face significant barriers accessing GPs,” said Lucy. “Metro based Viral Hepatitis Nurse Consultants are experienced in working with individuals remotely to enable them to access hepatitis C testing and treatment.
Aboriginal Health Practitioners Gordon Rigney (left) and Kelly Smith (photo by Beth Hummerston/Moorundi)
“We can arrange for blood tests, help interpret results, discuss results with patients over the phone, diagnose a hepatitis C infection and arrange for prescriptions if needed.
“We also check for other pre-treatment issues and support people through the treatment process and organise post treatment testing.
“These days, people don’t have to travel to a major centre to check their hepatitis C status or to get treatment. In South Australia, they can just call a Viral Hepatitis Nurse.”
National Picture
The objective of the National Australian HCV Point-of-Care Testing Program (HCVPOCT) is to scale up hepatitis C testing in higher risk and harder to reach communities including rural and Aboriginal communities, and prisons. One of the objectives of the Program is to see if increasing testing in targeted

communities will improve treatment uptake and completion.
Nationally, a total of 93 sites have registered including 27 prisons and 10 Aboriginal Community Controlled Health Organisation (ACCHO) sites. New South Wales leads the way with 44 sites, followed by Queensland with 23 and South Australia punching above its weight with 10.*
In South Australia, testing clinics have been held in prisons and drug and alcohol service locations.
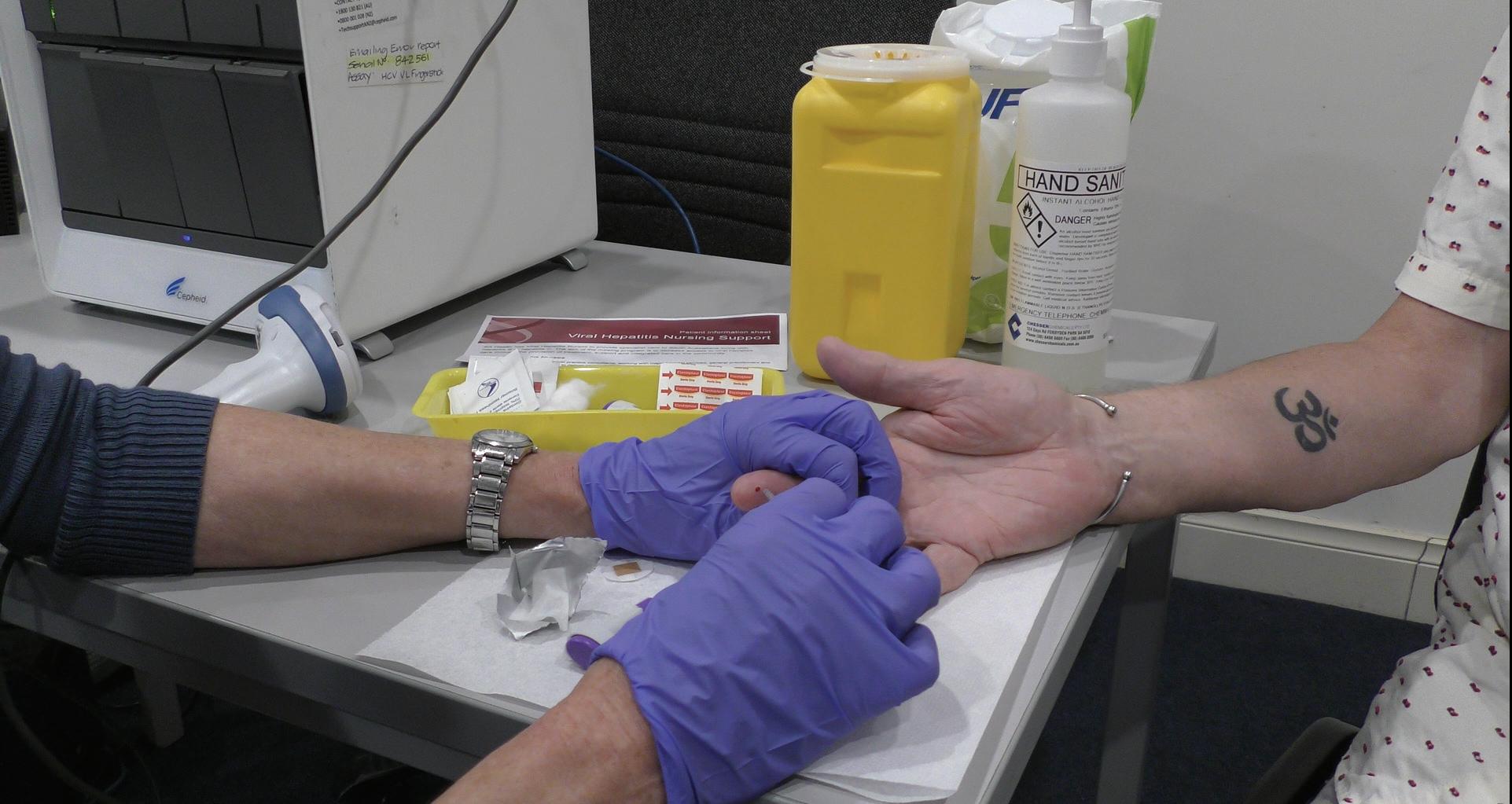
Point-of-care testing is done by taking a small drop of blood with a finger stick and processing it in a portable GeneXpert machine that provides results within an hour. The portability of the equipment means testing can be taken to the community, where people go regularly for other services.
 Viral Hepatitis Nurse, Lucy Ralton giving a rapid hepatitis C test to Kat Menz at the Barmera Pharmacy.
*Provided by The National Australian HCV Pointof-Care Testing Program, Coordinating Principal Investigator, Professor Jason Grebely.
Viral Hepatitis Nurse, Lucy Ralton giving a rapid hepatitis C test to Kat Menz at the Barmera Pharmacy.
*Provided by The National Australian HCV Pointof-Care Testing Program, Coordinating Principal Investigator, Professor Jason Grebely.
Each testing site is provided with a machine unless the service already has one. So far, 60 sites have started operating and 150 operators have been trained to operate the testing machines. Over 6,650 HCV pointof-care tests have been conducted via the Program with 850 people testing positive for chronic hepatitis C and 622 treated.
“Sites are often larger areas such as whole health districts and the operators move around the area. Operators do not normally work across different sites,” David explained. The impetus behind the National Hepatitis C Point-of-Care Testing Program is the decline in hepatitis C testing and treatment after the initial surge following the approval of new treatments in 2016.
The latest report from the Burnet and Kirby Institutes reveal that although over 95,300 people with hepatitis C had been treated between 2016 and the end of 2021, about 117,800 people still live with hepatitis C—a disease that can be cured in weeks with daily tablets.
An estimated 18% of those living with chronic hepatitis C were Aboriginal and Torres Strait people. In general, rural communities have less access to health information and services, having to deal with distance.

First Nations communities often deal with these same issues as well as additional cultural barriers.
Health workers who would like to help their clients access HCV point of care testing can find out more by calling 02 9385 0900 or emailing hcvpoct@kirby.unsw.edu.au.
Cecilia Lim
About the National Australian Point-of-Care Testing Program
The National Australian HCV Point-ofCare Testing Program is run by The Kirby Institute, UNSW Sydney and the International Centre for Point-of-Care testing at Flinders University. It is funded by the Australian Government Department of Health and Aged Care .

The objective of the Program is to establish a network of sites to scale up point-of-care HCV testing in settings which provide services to people at higher risk of hepatitis C, in order to increase testing and linkage to treatment.
The Program will be the first internationally to evaluate whether increasing point-of-care HCV RNA testing will improve treatment uptake among people at-risk of HCV.
It will contribute to understanding barriers to scaling up testing and treatment uptake, and inform HCV elimination efforts in Australia and globally.
Prisons: the weakest link in the fight against BBVs
Australian policy makers must act to reduce the spread of blood-borne viruses (BBVs) in prisons or we won’t be able to achieve critical public health goals like eliminating hepatitis C. This was the call in a consensus statement released by the Harm Reduction in Prisons Working Group.
The statement outlines an evidence-based approach to reducing the spread of BBVs and other injecting-related harms in prisons. Calling on policy makers to act, Australian Alcohol and other Drugs Council (AADC) CEO and consensus statement signatory, Melanie Walker, said. “The spread of BBVs in prison settings is currently like a hole in the rabbit proof fence of our National BBV and Sexually Transmissible Infections (STI) Strategies and this consensus statement outlines how we can work together to fix this gaping hole.
“The number and breadth of organisations represented by signatories to this consensus statement is significant. What we all agree on is that it’s really important that the full range of harm reduction options that are available in the broader community are mirrored in custodial settings if we are to successfully achieve public health outcomes for all.”
Director of the Drug Policy Modelling Program at UNSW Sydney and consensus statement signatory, Professor Alison Ritter, AO, said drug use and the spread of BBVs in prisons affect everybody because people who leave prison go back into the community to their families and friends.
According to experts behind the statement, Australia has committed to eliminating hepatitis C by 2030, but right now prisons are the weakest link in the strategy to reaching this goal.
What is harm reduction?
Injecting drug use can result in a number of fatal or serious harms including overdose, BBV transmission and injecting-related injuries. But all three of these harms can be reduced and/or prevented through effective harm reduction programs.

Harm reduction involves helping people to improve their health through providing practical and non-judgmental support. This involves meeting people where they are at, acknowledging that abstinence is not the only way to reduce harms arising from drug use.
“There is a wealth of evidence that supports the effectiveness of harm reduction programs,” said Prof. Ritter AO. “Harm reduction is effective at reaching the most marginalised members of society who would otherwise not access healthcare and it has also been proven to improve prison safety for
10 HEPATITIS SA COMMUNITY NEWS 97
This article was first published on the HepSAY blog. Visit hepsa.asn.au/blog for more posts.
Why prisons?
Prisons are high-risk environments for the spread of BBVs due to the lack of access to new and sterile injecting equipment, which results in people sharing unsterile equipment. Consequently, people in prisons continue to experience higher rates of hepatitis C and HIV than the general population.
“Despite Australia being an international leader in the provision of Needle and Syringe Programs to the general public, we have fallen woefully behind by excluding people in custodial settings from accessing this vital and lifesaving service,” said Prof. Ritter AO.
Prison settings also provide an opportunity to engage people who have a history of injecting drug use with health and well-being services that they may not have previously been able to access in the community.

These interventions not only make prisons safer, they also help to ensure better health outcomes for the communities to which people are returning after their release.
Policy makers must act
Calling on policy makers to act, the statement pointed out that Australia won’t be able to achieve critical public health goals like eliminating hepatitis C when it’s ignoring people in prisons.
“From a public health perspective it doesn’t even matter whether you care about prisoner health or not. The fact is that people come in and out of prisons and go back out into the community – so failing to address the spread of BBVs in custodial settings is a broader public health concern that directly affects Australian families and communities,” says Ms. Walker.
The consensus statement will provide assistance to policy makers at all levels of government in applying a broad and comprehensive approach to harm reduction in, and outside of, prisons.
The Working Group is a national cohort of health practitioners, researchers, sector representatives and advocates and is convened by the Social Policy Research Centre’s Drug Policy Modelling Program at UNSW Sydney.
READ MORE:
You can find the full consensus statement at bit.ly/3YTzqKd
HEPATITIS SA COMMUNITY NEWS 97 11
10 Strategies to Reduce BBVs in Prisons

Programs to manage and regulate the provision of sterile injecting equipment to prisoners who inject drugs, tops the list of strategies outlined in a consensus statement released by the Harm Reduction in Prisons Working Group (HRPWG).
The statement aims to provide a clear, concise overview of evidence-based harm reduction interventions needed to reduce injecting-related harms in Australian prisons. Briefly the proposed interventions are:
Regulated provision of sterile injecting equipment to people who inject drugs –commonly known as Needle and Syringe Programs (NSP) or Clean Needle Programs (CNP). Evidence shows that CNPs work to reduce blood-borne virus transmission and are considered best practice with evidence from 10 countries showing they work just as well in prisons as they do in the community.
The lack of regulated access to sterile injecting equipment is associated with new blood-borne virus infections and reinfections among prison populations despite the provision of direct-acting antivirals. Regulating access to new sterile needles is also an important strategy in preventing injecting-related injuries and disease.
Overdose prevention sites that provide a safer place for people to inject drugs under the supervision of health professionals where overdose can be quickly reversed. They provide opportunities for contact and referral to other services. Evidence shows they reduce the risk of overdose and improve access to care.
Needle cleaning agents – Bleach is an effective agent against hepatitis C and HIV when it can be used properly to clean needles and syringes. Where people in prisons cannot access clean and sterile injecting equipment, needle cleaning agents should be provided.
Naloxone - Evidence shows that takehome naloxone programs which train participants to recognise overdose and administer the opioid reversal drug, reduces overdose deaths both in prison and in the high-risk period following release from prison.
Peer-led education and programs -
Peer educators are more credible and trusted source of information for people in prison. Extensive research shows that education programs in prison are more effective at reducing risky behaviours when developed and delivered by peers. Peer support programs and peer workers provide emotional support and practical information, such as supporting engagement in testing.
Opioid Agonist Treatment (OAT) is a cost-effective treatment that is associated with reductions in harmful drug use, bloodborne viral infections and death, both in the community and in prison. OAT has also been found to improve prison safety and reduce rates of re-offending among people in prison. Combined use of OAT with needle and syringe programs is more effective at preventing new blood-borne virus infections than just providing OAT alone.
Blood-borne virus (BBV) screening should be offered to everyone entering prison and then yearly and be voluntary. International research suggests that optout systems where screening is standard practice for everyone rather than opt-in, is best for maximum take-up of screening, as long as people are adequately informed of their right to refuse.
Hepatitis B virus (HBV) vaccination of all people in prison is recommended by the Australian Government. HBV immunisation reduces the pool of people infected with HBV thereby reducing the likelihood of transmission.
Hepatitis C virus (HCV) treatmentDirect Acting Antivirals (DAAs) are an approved medication that have special prescribing status so can be accessed by people in prison under Medicare. The provision of unrestricted access to DAAs
has cured nearly half of all people living with hepatitis C in Australia (from 2016 to 2020) and has reduced incidence of new hepatitis C infections in Australia.
However, DAA treatment is less effective as a prevention strategy in situations where there are high rates of risky injecting behaviour and other harm reduction is unavailable. It needs to be combined with effective primary preventative measures such as needle exchange programs to achieve hepatitis C elimination. HIV prevention and treatmentPre-Exposure Prophylaxis (PrEP) is a medication that prevents HIV acquisition and Post-Exposure Prophylaxis (PEP) is a course of medication that can be taken after potential exposure to HIV to prevent acquisition. Antiretroviral Therapy (ART) is an approved medication to treat HIV. PrEP, PEP and ART are funded on the Pharmaceutical Benefits Scheme.
The Working Group in its statement said the recommended interventions have application for all people at risk of injectingrelated harm, disease and death in prisons and hoped that the statement would assist policy makers at all levels of government in all jurisdictions to apply a broader lens to harm reduction and to understand why a comprehensive response is needed.

Aboriginal and Torres Strait Islander people have a high rate of liver disease compared to the non-Indigenous population - with hepatitis B and C being common causes.
It is important to increase access to culturally appropriate information to assist in raising awareness of transmission routes and to break down some of the barriers to seeking testing and treatment.
Below are some examples of resources that have been developed with local community knowledge and expertise. Note that these resources may be best suited for the communities that they were developed for as the language, knowledge and images may be specific to that area.
In Our Library

Aboriginal and Torres Strait Islander Resources
young people who learn that their Auntie May has recently contracted hep B. They explore how hep B is transmitted and share key prevention measures with their local community in a fun and creative way.
Storybook: bit.ly/auntiemay Video: bit.ly/auntiemayvideo
Hep B is everyone’s business LiverWell, Melbourne, 2022. 3 fold brochure.

Describes how hep B is transmitted and the effect it may have, how to protect yourself, testing, treatment and vaccination information - and how to stay healthy. Illustrated with artwork by Peter WaplesCrowe (Ngarigu.) bit.ly/hepb_business

Aunty May and the dodgy tattoo: further adventures of Iluka, Janalli, Miro and Bindi Carbal Creations and Hepatitis Queensland, Brisbane, 2022 Follows the journey of four
Win the fight against hep C LiverWell, Melbourne, 2022. 3 fold brochure.

Brochure with information about symptoms, testing, treatment, staying healthy and staying safe. Illustrated with artwork by Peter Waples-Crowe (Ngarigu.) bit.ly/fight_hepc
Better to know
Aust Federation of AIDS Organisations & Anwernekenhe National HIV Alliance, Sydney, 2022. Website

A sexual health resource for Aboriginal and Torres Strait Islander people. It provides information about common sexually transmitted infections (STIs), what to do if you have an STI and where to get tested. It contains information that deals with both men’s and women’s business. Includes a form to register for free email or SMS reminders for a sexual health check up.
bettertoknow.org.au
14 HEPATITIS SA COMMUNITY NEWS 97
Viral: are you the cure?
Melbourne Ilbijerri Theatre Company 2022. Video 26 minutes

A play that communicates hepatitis C prevention and education messages in a culturally appropriate way to the Indigenous community. It also aims to break down stigma and promote healing. Created through an in-depth engagement process, including community workshops and yarning circles bit.ly/viral_thecure
Hep C in 4

Hepatitis SA, Adelaide, 2021. Poster plus video 8:40 minutes. Poster for health workers in regional and country SAparticularly Aboriginal Health Workers: outlines actions for assessing, referring, informing and following up on Hepatitis related concerns. For ISSUU resources: may need to turn off ad blocker for full access. Also available: video of Aboriginal Health Council of SA (AHCSA) Sexual Health/BBV Program Coordinator, Joshua Riessen, introducing the guide.
Poster: bit.ly/hepcin_4
Video: bit.ly/hepcin4video
Inception Strategies comic books
Inception strategies Sydney, various dates. Set of graphic booklets/comics
A series of comics focusing on health literacy for Aboriginal communities: concentrating on general health, liver health, blood-borne viruses and sexual health. Inception Strategies develop comic scripts via workshops with local community groups.

Powerful and free: an honest conversation about hepatitis B

Hepatitis Queensland, Brisbane, 2022. Video 5:19 minutes
Tells the story of Bec’s experience with hep B. Since her diagnosis Bec has found there is a lack of understanding about hep B - both from health care providers and Indigenous community: “It’s travelled through the generations and many barriers stand in the way of access to treatment which must be broken down before we can begin to address how the virus is transmitted and what it means to be a carrier”.
bit.ly/powerful_honest
(This film is part of Hepatitis
Queensland’s B Stronger campaign which can be found at bit.ly/b_stronger)
Love Your Liver: nyuntumpa

alu wiru kanyinma
Hepatitis SA & Aboriginal Health Council of SA, Adelaide, 2014. An illustrated bi-lingual step by step guide, covering hep B transmission (and how it’s not spread), living healthy with hep B, pregnancy – and general liver health tips. For use by health workers with their clients. For ISSUU resources: may need to turn off ad blocker for full access. Hard copies available (email admin@hepsa.asn.au). bit.ly/loveyourliver_pitj
Catalogue list with additional information and links: bit.ly/ inception_hepsa
To see a listing of all available resources on this topic, visit bit. ly/hepsa_list.
HEPATITIS SA COMMUNITY NEWS 97 15
Hepatitis SA provides free information and education on viral hepatitis, and support to people living with viral hepatitis.
Postal Address: Kaurna Country PO Box 782
Kent Town 5071
(08) 8362 8443



1800 437 222
www.hepsa.asn.au
HepSAY Blog: hepsa.asn.au/blog
Library: hepsa.asn.au/library
@HepatitisSA
@hep_sa
Resources: issuu.com/hepccsa

Email: admin@hepatitissa.asn.au
HEPATITIS SA BOARD



Chair

Arieta Papadelos
Vice Chair
Bill Gaston Secretary
Sharon Eves Treasurer
Michael Larkin
Ordinary Members
Catherine Ferguson
Bernie McGinnes
Sam Raven
Joshua Reissen
Salma Safi
Kerry Paterson (CEO)
Free hepatitis A, B and C information, confidential and non-judgemental support, referrals and printed resources.
We can help. Talk to us. Call or web chat 9am–5pm, Mon–Fri
Information Support

1800 437 222
hepsa.asn.au

Hepatitis SA has a wide range of hepatitis B and hepatitis C publications which are distributed free of charge to anyone in South Australia.
To browse our collection and place your orders, go to hepsa.asn.au/orders or scan the QR code below:

16 HEPATITIS SA COMMUNITY NEWS 97
Because it is the only one you have and you can’t How Do I Love My Liver? Pr and alcohol. egular ex educe alcohol intak standar oid binge drinking don’ Why Love My Liver? Why Love My Liver? or hepatitis and B to find out more. Hepatitis Hepatitis SA provides information, support and education to people affected by hepatitis, and health and community work Because it is the only one you have and you can’t live without it! How Do I Love My Liver? er against main Why Love My Liver? Why Love Liver? Get accinated or hepatitis and tooing and other pr equipment not to find out more. 3 y g 1300 437 222 Hepatitis SA provides information, support and education to people affected by hepatitis, and health and community work you have and you can’t live without it! How Do I Love My Liver? Why Love My Liver? Why My Liver? tooing and other pr y g 1300 437 222 p Hepatitis SA provides information, support and Keeping up your exercise regime can sometimes be Don’t let yourself get bored—try different Promise yourself healthy rewards (perhaps Exercise with partner or group. Having 437 222 or visit Hepatitis SA online at hepatitissa.asn. explore the catalogue online at hepsa.asn.au/library health.gov.au/internet/main/publishing.nsf/content/healthartwork Hana Jang, used under Creative Commons license: [flickr.com/photos/from_drawing] Exercise for Healthy Livers SAHealthhascontributedfundstowardsthisProgram. Once you’re comfortable with this, you can too hard, you might end up feeling overtired or run-down, which can make you more likely altogether and undo all the work things off, but then you run the risk of giving (perhaps high-quality healthy treats, or harder for you to drop out, and you can that it becomes a normal part of your Hepatitis SA has lots of useful information Visit our library online at hepsa.asn.au/ the Australian National Physical Activity The Heart Foundation has number of helpful Exercise for Healthy Livers Hepatitis SA towards this Program. Fibroscan What is it, and how will it help me? Hepatitis SA www.hepatitissa.asn.au What are the risks? fibroscan. Fibroscan scores are very useful tool, but they are not the whole picture. Your doctor or nurse will take into account all the information they have about your health when they make recommendations to you about your treatment options, not just the scan results. how isapplied 1800 437 222 hepsa.asn.au Support Living with Advanced Liver Disease Helpful Hints § Gum Infections Infected gums bleed when brushed, or may swell or redden. Receding gums, loose teeth and bad breath are also symptoms of gum infection. Decay, above) Using interferon (occasionally used as treatment for hepatitis C) or smoking can lower your resistance to gum disease holding the brush at 45° to the gum line and moving the brush in small circles Use dental floss on the gaps between teeth and on the surfaces of teeth Use an antibacterial mouthwash, preferably alcohol-free (like PerioGard) Denture Care each meal, and clean them daily with a soft brush and mild soap. Don’t use toothpaste, as this will wear the dentures away. Dentures should be removed at night and left to soak in cold water while not in Warning People with cirrhosis or blood/ bleeding disorders, or who are taking interferon, should talk to dentist about any special precautions which may be Hepatitis C & Dental Care C Cartoon The Divine Harvester Hepatitis SA (08) 8362 8443 Kaurna Country Hepatitis C Treatment There are highly effective cures for hepatitis or no side effects. These drugs, known as direct acting antivirals, are available on the Pharmaceutical Benefits Scheme (PBS). Hepatitis C Information for Family & Friends
Viral Hepatitis Community Nurses
Viral Hepatitis Nurses are nurse consultants who work with patients in the community, general practice or hospital setting. They provide a link between public hospital specialist services and general practice, and give specialised support to general practitioners (GPs) to assist in the management of patients with hepatitis B or hepatitis C. With advanced knowledge and skills in testing, management, and treatment of viral hepatitis, they assist with the management of patients on antiviral medications and work in shared care arrangements with GPs who are experienced in prescribing medications for hepatitis C or accredited to prescribe section 100 medications for hepatitis B. They can be contacted directly by patients or their GPs:
CENTRAL: QUEEN ELIZABETH HOSPITAL
Jeff: 0423 782 415
Debbie: 0401 717 953
NORTH
Bin: 0401 717 971
Specialist Treatment Clinics
SOUTH Rosalie: 0466 777 876
Lucy: 0466 777 873
OFFICE: (08) 8204 6324
Subsidised treatment for hepatitis B and C are provided by specialists at the major hospitals. You will need a referral from your GP. However, you can call the hospitals and speak to the nurses to get information about treatment and what you need for your referral.
• Flinders Medical Centre Gastroenterology & Hepatology Unit: call 8204 6324
• Queen Elizabeth Hospital: call 8222 6000 and ask to speak a viral hepatitis nurse
• Royal Adelaide Hospital Viral Hepatitis Unit: call Anton on 0401 125 361
• Lyell McEwin Hospital: call Bin on 0401 717 971
Don’t like Talking? No Problem.
Visit hepsa.asn.au - no need to log in, lots of info & pdates
Follo the HepSAY blog - hepsa.asn.a /blog
Order print resources - hepsa.asn.a /orders/
Follo s on T i er @hep_sa or Facebook @Hepa sSA
ALL ser ices & reso rces FREE
Blood-Safety Education
Update your knowledge on blood-safety and viral hepatitis. Sessions include:

Over view of hepatitis A , B & C
Blood and bodily-fluid safety
Best practice after blood exposure
Stigma and discrimination
Available ser vices
FREE 1.25 HOURS =
TUE 4 APR 2023, 11 AM - 12:15 PM

MON 8 MAY 2023, 12 - 1:15 PM
WED 14 JUN 2023, 11 AM - 12:15 PM
Funded by SA Health. Brought to you by Hepatitis SA E D U C AT I O N @ H E P S A . A S N . A U Q U E S T I O N S ?
VIA: W W W.T R Y B O O K I N G .CO M / C DV S F
BOOK