

March 2024 www.mforum.com.au Surgery & pain management | Perioperative clinics, botulinum for pain, arthrofibrosis & opioids Pain relief on the books MAJOR PARTNERS

*Terms and conditions apply. Must join by 8 April 2024 on combined hospital and extras cover to receive 8 weeks free and 2-month waiting periods on extras waived. New members only. Check eligibility in the full terms and conditions at www.doctorshealthfund. com.au/8weeksfree. IMPORTANT: Private health insurance products are issued by The Doctors’ Health Fund Pty Limited ABN 68 001 417 527, a member of the Avant Mutual Group. Cover is subject to the terms and conditions (including waiting periods, limitations and exclusions) of the individual policy, available at www.doctorshealthfund.com.au/our-cover. DHF 406_3/24 Dr Rebecca Barnes Member since 2011 Join on any hospital & extras by 8 April*. Plus, skip the two-month waits on extras. Switch today 1800 226 126 doctorshealthfund.com.au 8

One man’s pain is society’s gain
New generations of doctors will now get a much-needed insight into managing the thousands of chronic pain patients they will see coming through their doors in the years ahead.
Chronic pain is a pain in the neck, sometimes literally.
Unlike the short-term acute pain from twisting an ankle, chronic pain – as the name suggests – can linger indefinitely.
Telling a patient that they might have pain for a long time – maybe forever – is hard message for any doctor to deliver.
Many patients will assume that there is now a fix for everything – a tablet or treatment that will take away the pain. The idea of learning to live with some level of discomfort is abhorrent.
For retired Perth businessman Geoff Churack, who was struggling with ongoing leg pain in the early 2000s, a lack of awareness about managing chronic pain – even among the GPs he was seeing – left him frustrated.
Geoff, who is on this month’s cover, wanted to do something about it, providing $1 million in 2013 to set up the Churack Chair in Chronic Pain Education and Research at Fremantle’s University of Notre Dame.
A decade later, with the early work starting to pay off, Geoff and his family have now dug deeper, providing another $4 million to ensure the work they started can continue in perpetuity.
Geoff has always known that while he might not personally benefit from the research and education, many other people might.
New generations of doctors will now get a much-needed insight into managing the thousands of chronic pain patients they will see coming through their doors in the years ahead.
Kudos to the Churack family.
SYNDICATION AND REPRODUCTION Contributors should be aware the publisher asserts the right to syndicate material appearing in Medical Forum on the mforum.com.au website. Contributors who wish to reproduce any material as it appears in Medical Forum must contact the publisher for copyright permission.
DISCLAIMER Medical Forum is published by Medforum Pty Ltd (Publisher) as an independent publication for health professionals in Western Australia. Neither the Publisher nor its personnel are medical practitioners, and do not give medical advice, treatment, cures or diagnoses. Nothing in Medical Forum is intended to be medical advice or a substitute for consulting a medical practitioner. You should seek immediate medical attention if you believe you may be suffering from a medical condition.
The support of all advertisers, sponsors and contributors is welcome. To the maximum extent permitted by law, neither the Publisher nor any of its personnel will have any liability for the information or advice contained in Medical Forum. The statements or opinions expressed in the magazine reflect the views of the authors and do not represent the opinions, views or policies of Medical Forum or the Publisher. Readers should independently verify information or advice. Publication of an advertisement or clinical column does not imply endorsement by the Publisher or its contributors for the promoted product, service or treatment.
Advertisers are responsible for ensuring that advertisements comply with Commonwealth, State and Territory laws. It is the responsibility of the advertiser to ensure that advertisements comply with the Competition and Consumer Act 2010 (Cth) as amended. All advertisements are accepted for publication on the condition that the advertiser indemnifies the Publisher and its personnel against all actions, suits, claims, loss or damages resulting from anything published on behalf of the advertiser.
EDITORIAL POLICY This publication protects and maintains its editorial independence from all sponsors or advertisers. Medical Forum has no professional involvement with advertisers other than as publisher of promotional material. Medical Forum cannot and does not endorse any products.
MARCH 2024 | 1 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
EDITORIAL Cathy O’Leary | Editor
BACK TO CONTENTS
Inside this issue



1
4
8 In brief
29
35
48
Cover
BUMPER COMPETITION TIME
The lucky winner of our January doctors dozen from Capel Vale is Dr Frank Willis
This month, we have another premium selection of wine to win –from Duke’s in the Porongurups, reviewed by Dr Martin Buck on page 53. Medical Forum also has a bumper movie giveaway, with 22 double in-season passes to three new movie releases, with all the details on page 51.
2 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT CONTENTS | MARCH 2024 – SURGERY & PAIN MANAGEMENT IN THE
NEWS
Editorial: One man’s pain is society’s gain – Cathy O’Leary
News & views
26 DNA unearths ancient health songlines
Hearing and dementia studied
The numbers tell a story – Dr Joe Kosterich
Shock over clinic closure
image:
Churack Courtesy of University of Notre
Geoff
Dame
10 14 22
FEATURES
Cover story: Churack family’s lasting legacy
Close-up: Dr Sanjay Mukhedkar
Is there a doctor in the House? 22 Aligning robots and business LIFESTYLE
When the chef met the surgeon 52 Medicine made funny 53 Wine review Duke’s – Dr Martin Buck 54 Heat shelters are cool WINPREMIUM WINESFROMDUKE’ S V I N DRAYE 18 CONNECT WITH US /medicalforumwa /MedicalForum_ /medical-forum-wa-magazine info@mforum.com.au www.mforum.com.au
To win the wine or the movie tickets, use the QR code on this page, or go to www.mforum.com.au and hit the competitions tab.
10
14
18
50
PUBLISHERS
Fonda Grapsas – Director
Tony Jones – Director tonyj@mforum.com.au
EDITORIAL TEAM
Editor Cathy O'Leary 0430 322 066 editor@mforum.com.au
Production Editor
Jan Hallam 08 9203 5222 jan@mforum.com.au
Journalist
Eric Martin 08 9203 5222 eric@mforum.com.au
Clinical Editor
Dr Joe Kosterich 0417 998 697 joe@mforum.com.au
Graphic Design Ryan Minchin ryan@mforum.com.au
ADVERTISING
Advertising Manager
Andrew Bowyer 0424 883 071 andrew@mforum.com.au
Clinical Services Directory
Alice Miles 08 9203 5222 alice@mforum.com.au
CONTACT MEDICAL FORUM
Suite 3/8 Howlett Street, North Perth WA 6006
Phone: 08 9203 5222
Fax: 08 6154 6488 Email: info@mforum.com.au www.mforum.com.au














MARCH 2024 | 3 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
OUR PRINTER’S ACCREDITATIONS CONTENTS This magazine has been printed using solar electricity, and the paper is manufactured with elemental chlorine-free pulps. Both printer and paper manufacturer are certified to ISO 14001, the world’s highest environmental standard. Environment ISO 14001 MAJOR PARTNERS Clinicals 36 Strategies for implementing perioperative clinics Dr Steve Same 39 Recurrent abdominal pain in children Dr Amit Saha Guest Columns 30 Misunderstood weight loss needs unravelling Dr Vanessa Vaughan 33 Changing eating behaviours is a journey Hayley Breare, Prof Barbara Mullan, Dr Chloe Maxwell-Smith & Prof Deborah Kerr 45 Botulinum toxin type A in pain management Dr Jie Xiu 46 Common inguino-scrotal lumps and bumps in kids Dr Michael Collin 48 Arthrofibrosis –a common side effect of joint surgery Kayley Usher PhD 40 Interventional pain management for knee arthritis Dr Reza Feizerfan 42 Advancements in managing spinal pain A/Prof Greg Cunningham 43 Opioid and benzo prescribing in chronic pain Dr Chris Martin
Breathing easy for early arrivals
A Perth study is underway to help people born preterm to breathe easier.
Chronic lung disease is a common outcome, but Curtin University research is working to improve life for them, regardless of their age.
The project, known as FINGERPRINT, has been awarded nearly $2 million over five years from the Medical Research Future Fund. The research team will use sophisticated machine learning to better understand the different types of lung disease affecting more than half of people born preterm, to create more effective treatments and better predict those at risk of developing lung conditions.
Preterm lung disease has features of asthma and chronic obstructive pulmonary disease and is often managed with similar treatments, as there is no evidence-based guidance on how to treat preterm respiratory disease specifically.
The FINGERPRINT project aims to address this by distinguishing the different types of preterm lung disease to develop phenotypes — or ‘fingerprints’ — which are individual identifiers that will allow researchers to develop targeted, personalised treatments.
Study lead Associate Professor Shannon Simpson, from Curtin School of Allied Health and Telethon Kids
Boom time for WA health jobs
Western Australia has emerged as the State with highest demand for medical jobs, with a 4.1% rise in vacancies in the last quarter of 2023, while most States went backwards.
An analysis by healthcare recruiter Omega Medical shows there was a 2.2% increase in demand for jobs across all healthcare sectors in Australia.
The standout feature in its Jobs and Salary Index was a strong 17.5% rise in medical practitioner job vacancies. This surge, along with a year-on-year rise of 15.5%, indicates a critical shortage, despite a net migration of 500,000 nationally.
General practice jobs rose by 6.4% in the quarter, closely correlating with the reported increase in GP and practice management positions.
Nursing job opportunities experienced a slight dip of 2.1%, primarily due to the normalisation

Institute, said this individualised approach was vital in identifying appropriate and tailored treatment options for a vulnerable group of people.
“People born preterm are five times more likely to be diagnosed with asthma, are over-represented in adults with COPD or pulmonary hypertension and we have even recently seen the first case of lung transplant in young adults who were born pre-term,” she said.
“We believe phenotype traits of lung disease will be ‘expressed’ to varying degrees between individuals born significantly preterm, which can be targeted to develop personalised treatments.”
Another key aspect of the study is helping to predict which babies born preterm will develop lung disease later in life.
The study is between Curtin and Wal-yan Respiratory Research Centre — a partnership between Telethon Kids Institute, Perth Children’s Hospital and Perth Children’s Hospital Foundation — and other contributors.
of job volumes following the pandemic-induced surge.
Salaries and hourly rates are anticipated to remain at historically high levels, according to Omega Medical’s Managing Director John Codner.
"Our Quarter Four 2023 Index demonstrates the resilience of the Australian medical employment market and the ongoing need for all types of medical and allied healthcare professionals across the country,” he said.
“We need more support from our government and education institutions to address this crisis, which is only getting worse every year as our population increases and on average grows older.”
All sub-sectors showed growth except for aged care (down 2%) and hospitals (down 1.5%). The fall in aged care was attributed to the earlier one-off push to hire registered nurses in aged care facilities in some States.
Testing times for app
The Royal College of Pathologists of Australia has launched the 8th edition of its flagship publication, the Manual of Use and Interpretation of Laboratory Tests, along with a mobile app.
Popularly known as 'The Manual', it has more than 500 pathology entries, including updates to 488 existing pathology test entries and 559 topic entries.
It has also archived 78 outdated test entries and added 62 new entries.
The new mobile app designed to complement The Manual allows for offline use and provides better accessibility, particularly for healthcare professionals working in remote and regional locations.
Clinical Professor John Burnett, RCPA Fellow and editor of The Manual, said the companion app was a significant leap forward in
continued on Page 8
4 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
NEWS & VIEWS
BACK TO CONTENTS



MARCH 2024 | 5 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT MAJOR PARTNER From sample collection to results, your patients are safe with us Prof. Catherine Cole Dr Clay Golledge Biochemistry & Toxicology Dr Jonathan Grasko Dr Yael Grasko Immunology Dr Martin Stuckey Dr Meilyn Hew Saturn Pathology | Level 2, 31 Cedric Street, Stirling 6021 | Phone: (08) 9253 4800 www.saturnpathology.com.au Laboratory Medicine Redefined BACK TO CONTENTS

MAJOR PARTNER BACK TO CONTENTS

BACK TO CONTENTS
continued from Page 4
efforts to provide up-to-date and accessible resources for healthcare professionals.
“The Manual is particularly useful for GPs, providing them with updated and comprehensive information to make informed decisions about pathology testing,” he said. “With the new app's offline functionality, GPs in remote and regional areas can access critical information even without internet connectivity, enhancing their ability to deliver quality care."
Study finds high RSV awareness
A Telethon Kids Institute study to gauge community awareness of respiratory syncytial virus has found parents are open to immunisation to tackle it.
RSV is a common respiratory infection affecting babies that can lead to bronchiolitis and pneumonia.
The virus is responsible for 3.6 million infant hospitalisations and 100,000 deaths globally, sparking a push for vaccines and antibody treatments that are now just around the corner.
An antibody treatment called Nirsevimab, which protects babies
IN BRIEF
Chemical pathologist and AMA WA president Dr Michael Page is new CEO of Clinipath Pathology.
St John of God Murdoch Hospital has made Dr Tessa Blom its permanent head of emergency medicine – the role she has been acting in for six months.
for up to five months during peak RSV season, was approved by the Therapeutic Goods Association in December last year and is expected to be rolled out in Australia over the next year.
Of the 1,992 participants in the national online survey, most aged 25-39 years, 89% of current parents and 78% of pregnant and planning parents knew about RSV.
But despite high awareness of the virus itself, the study showed low awareness of associated conditions and disease severity, suggesting a need for targeted education campaigns to fill the knowledge gap.
Lead author Charlie Holland, from the Wesfarmers Centre of Vaccines and Infectious Diseases based at TKI, said the findings signalled the need to further raise awareness about RSV before any immunisation rollout.
Drug dangers for over-65s
Perth researchers have helped to develop an Australian-first list of 16 potentially dangerous medications for over-65s and safer alternatives.
Involving RMIT and UWA, researchers identified potentially inappropriate medicines (or PIMs) with risks that may outweigh their benefits. PIMs can have high risks of severe adverse effects, drug


Telethon Kids Institute has launched Inklings, a world-first program for babies with delays in their social and communication skills, with support from the NDIS.
interactions, increased risk of falls and death.
Around the world, lists of these risky medicines are used to help health professionals improve medication management and safety.
Lead researcher, Dr Kate Wang, said PIMs lists helped clinicians identify medications that had higher risk of negative clinical outcomes, including hospitalisation and death.
“They should only be used in circumstances where there is a clear need and not an effective and lower-risk alternative available,” she said.
“The Australian setting is unique, and it is vital that we have our own, up-to-date resource.”
These lists of high-risk medicines were especially important for older people, who often needed multiple medications to manage their conditions. Between 20-70% of older people are prescribed at least one PIM.
The study drew on a multidisciplinary expert panel of 33 clinicians and researchers with expertise in geriatrics, general medicine, pharmacy, clinical pharmacology, general practice and epidemiology.
Narelle Supanz, a long-time practice manager for GPs and specialists, was recently awarded life membership with the Australian Association of Practice Management.

Construction is underway on WA’s first children’s hospice, the $34 million Boodja Mia project, in Swanbourne.
Professor Kirsten Auret, WA Country Health Service Clinical Director of Palliative Care, was awarded a Member of the Order of Australia in this year’s Australia Day honours for her service to palliative care medicine and tertiary education.

8 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT NEWS & VIEWS
BACK TO CONTENTS
Hospital upgrade underway
St John of God Health Care has signed Multiplex to build the next stage of upgrades to its Subiaco hospital.
Hospital CEO Tina Chinery said the works would improve the patient and visitor experience, revitalise and replace ageing infrastructure and prepare the campus for new clinical facilities.
“This includes modernising the main entrance and lobby, replacing patient lifts across the campus, improving visitor parking and upgrading ageing infrastructure to ensure continuity of service,” Ms Chinery said.
The works are expected to continue until mid-2026, with the redevelopment of the Subiaco hospital spanning several stages.
Stage one works were completed in January this year, including an upgrade to the kitchen, new service lifts and a six-bed negative pressure isolation ward.
Stage two engineering and enabling works include an upgrade to the main hospital entrance and lobby, including a new reception counter, floor finishes and digital signage; the replacement of patient lifts across the campus; and upgrades to the existing multi-storey carpark and engineering services.
A decision on stage three is expected later this year, with plans for a new eight-storey clinical building with a mother and baby centre, heart centre, six operating theatres and a new chapel.
Hoping for a stroke of luck
A Perth stroke expert has described as alarming predictions of a 50% increase in stroke deaths and a 30% increase in related disability worldwide by 2050.
The finding comes from an international commission by The Lancet Neurology, in collaboration with the World Stroke Organisation and the World Health Organization, to understand and tackle the global burden of stroke.
Distinguished neurologist Professor Graeme Hankey, Perron Institute Chair of Stroke Research at UWA, is a member of the commission’s steering committee and the WSO Implementation Task Force on Stroke.
Stroke is the second leading cause of death and the third leading cause of disability (which includes depression and dementia) in 2020. The burden of disability after a stroke is increasing faster


in low-income and middle-income countries.
The absolute number of people affected by stroke has almost doubled in the past 30 years, and the incidence of stroke in people younger than 55 years is increasing.
The work of the commission began seven years ago, with the aim of improving surveillance, prevention, acute care and rehabilitation, while involving clinicians, health providers, policymakers and
researchers to combat the rising burden of stroke.
“The predicted trajectory for the impact of stroke on global health and its economy is alarming,”
Professor Hankey said.
“However, as the international commission found, there are opportunities to reduce the burden of stroke, particularly in parts of the world where the required resources are lacking.
“Among other recommended measures are prevention strategies for people at risk of cerebrovascular disease, with an emphasis on early detection and control of high blood pressure.”
Professor Hankey said priorities included more acute stroke services, interdisciplinary stroke care services, workforce training, capacity building for community health workers in stroke rehabilitation and monitoring of quality indicators for stroke services.
MARCH 2024 | 9 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
NEWS & VIEWS BACK TO CONTENTS

Perth family’s pain relief for doctors
Medical Forum editor Cathy O’Leary first spoke to retired car dealer Geoff Churack in 2013, when he boldly put up $1 million to better equip WA doctors to help patients struggling with chronic pain. Now, a decade later, he has just made one of the biggest donations of its kind in Australia, to keep this education going permanently.
COVER STORY
BACK TO CONTENTS 10 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
Moira and Geoff Churack with daughters Danielle, left, Simonne and Emma
WA’s medical profession has five million reasons to thank a retired Perth businessman and his family when it comes to better understanding and treating chronic pain.
Geoff Churack and his wife Moira, supported by their three adult daughters, have donated $5 million to the University of Notre Dame and its school of medicine – the biggest gift in the university’s history and one of the largest philanthropic donations of its type in Australia.
The money will be used partly to better educate doctors and medical students in the area of chronic pain, which costs the Australian economy $35 billion a year in lost productivity as well as making life a misery for many people.
During his working life, 85-yearold Mr Churack owned and operated several highly successful car dealerships across WA. In more recent years, he has been fighting his own battle with chronic pain, living with the debilitating condition, complex regional pain syndrome (CRPS).
There is no cure for CRPS, which leaves sufferers in almost constant and, at times, excruciating pain.
After his diagnosis, Mr Churack did the rounds of doctors to try to get relief from crippling aches in his leg, which he blamed on sports injuries in his younger days and unsuccessful back surgery for his chronic neuropathic pain.
Knowledge gap
But he was surprised by how little his doctors knew about chronic pain and the long-term effects it can have on mental health and wellbeing.
Chronic pain is defined as constant daily pain for three months or more in the past six months. The most common types are osteoarthritis and back issues, followed by musculoskeletal problems, other arthritic conditions and cancer.
Instead of feeling defeated, Mr Churack and his wife decided to help change the local landscape in how chronic pain was managed in the hope it could also bring relief to some of the 3.5 million Australians affected by it.
The couple initially donated $1 million to Notre Dame in 2013
to establish the Churack Chair of Chronic Pain Education and Research, in partnership with St John of God Subiaco Hospital. The key inaugural position was filled in 2015 by pain specialist Professor Eric Visser.
The family has now given another $4 million to permanently endow the chair role.
Notre Dame Vice Chancellor Professor Francis Campbell said the family had made an extraordinary gift to its school of medicine, in turn helping those who live with chronic pain and who were desperate for a breakthrough that could help reduce their suffering.
“This gift will ensure the Churack Chair can continue to focus on improving education and awareness about chronic pain, particularly among medical professionals,” Professor Campbell said.
“A PhD study funded by the Chair found that Australian medical students spent just 20 hours on average learning about the causes and treatment of pain during their training.
“Notre Dame’s school of medicine has since amended its syllabus to include a much stronger focus on chronic pain, which includes having our students spend time at St John of God Subiaco Hospital’s pain management service.
“These are important developments that ensure our graduates enter the workforce equipped with increased levels of knowledge, empathy and compassion to be able to assist those living with chronic pain.”
Mr Churack said that in the early days of his battle with pain, it
continued on Page 12

MARCH 2024 | 11 COVER STORY
BACK TO CONTENTS
Perth family’s pain relief for doctors
continued from Page 11
became clear that the problem began in medical schools, which had traditionally placed very little emphasis on teaching their students about the physical and emotional impacts that chronic pain can have on a patient’s life.
“That is why I reached out to Notre Dame, knowing that they operate one of Australia’s leading medical schools, to see what we could do together to improve research and training in these areas,” he said.
“We were very fortunate to secure renowned WA pain specialist, Professor Visser, as our inaugural Chair, and we have already achieved a great deal under his leadership.
“But there is still so much more that needs to be done, which is why my family and I have decided to invest these additional funds to enable Eric and his team to continue their efforts for many years to come.”
Welcoming the endowment, SJOG Subiaco Hospital Chief Executive Officer Tina Chinery said the hospital played an important role in developing the next generation of medical professionals coming through Notre Dame.
Experts onboard
“Our pain management team includes the largest cohort of accredited pain specialists in WA, who enjoy sharing their knowledge, skills and experience with Notre Dame’s medical students,” Ms Chinery said.
“It gives those students exposure to the latest diagnostic and treatment options being used by specialists who are leaders in their field.”
One of the Churacks’ daughters, Simonne Ventouras, paid tribute to her parents, describing their $5 million gift as an incredible legacy that was already making a real difference to the lives of people with chronic pain.
“My sisters Emma, Danielle and I are all so incredibly proud of Mum and Dad and we look forward to working closely with the Chair to ensure it continues to deliver highquality education outcomes in this

important area of medicine,” Mrs Ventouras said.
In addition to training medical students, the Churack Chair supports research by masters and doctoral students from the university. Staff also work with other leading research institutions on clinical trials and other projects. Professor Visser is currently involved in the largest-ever study of potential treatment options for CRPS, which is testing a new medication and brain retraining techniques. He also teaches at Notre Dame in addition to running his own private practice.
He said the impact of chronic pain on the broader community was immense in terms of lost productivity.
“But it is the human cost for those individual sufferers that is even greater, with pain making it impossible for many to carry out even the most basic of household chores, or even get out of bed,” he said. “That’s why research and education are so important.
“Research-wise, the major projects we’ve been involved with, working
cooperatively with teams, initially at Murdoch University and then through the colleges, have been on nerve pain, neuropathic pain, and pain associated with lumbar nerve compression – the classic sciatica pain.
“We’ve got some good studies on migraine and basic science. There’s pretty limited basic pain science research in Australia, so part of the Churack chair was to support some of that work, particularly with nerve pain.
“The second thing we’ve done is some clinical trials, and we’ve found that some vitamin therapies can be helpful in reducing the risk of migraine, and we’re doing this concurrently with Curtin University.
“We’re also doing a big study with NeuRA (Neuroscience Research Australia) in NSW into treatments for nerve pain, not just medications but neuro and physiotherapy treatments, so a lot’s been happening in the research space.”
Equipping students
Professor Visser said the main focus in education was medical students, but he was involved in education at all levels at Notre Dame, as well
12 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
COVER STORY
BACK TO CONTENTS
Professor Francis Campbell, Moira and Geoff Churack and Professor Eric Visser
the other universities when they attended the hospitals.
“One of the PhD’s research is about students’ pain education – how to improve education and outcomes for medical students, how to best train them on pain, which is a core thing, so it’s been instigated into the curriculum, and it’s getting a profile in the examinations,” he said. Traditionally, chronic pain did not have a big presence on the medical curriculum.
Professor Visser said one of the program’s PhD students found that in Australasia about eight or nine years ago, less than 5% of curriculum time had a pain focus to it – even though in all aspects of medicine, from psychiatry to surgery to general practice, a big component of their work was in pain.
“That was a key finding from
Australasia and around the world that there was minimal pain content in the curriculum and considering that at least 20% of doctors’ caseload has a significant pain issue, there is certainly a disconnect between that and what’s actually taught.
“We haven’t measured it yet, but it’s a very strong impression that the newer cohorts graduating from all the WA universities – and we can certainly speak for Notre Dame – definitely have a much clearer core understanding of pain and complex things such as using opioid medicines safely.
“So, compared to my days as a medical student, they’re getting the message and there’s a lot more exposure to pain.”
For GPs too
Professor Visser recently spoke to
dozens of GPs in Albany about pain management topics, particularly the appropriate use of opioids and analgesics in pain management.
“We also spend a lot of time in GP education, and one of the projects we will be looking at is targeting education at the newly-graduated doctors – the interns and the RMOs – because that definitely needs some attention,” he said.
“We’ll be working with senior medical students and junior doctors, to give them practical modules to get them graduation-ready in terms of pain management.”
Professor Visser said the significance of the recent endowment was that it would perpetuate the current work and allow it to expand. Notre Dame was doing a lot of cooperative work with Murdoch, Curtin and other universities, which was vital for long-term success.
“It prolongs the work, which we’re really only getting started on, and will also allow us to have more academic appointments and to work with allied health, because we’re not just talking about doctors and medical students,” he said.
“And with the extra funding, we can reinstate our basic science research post-doc that we had for some time before the funds came to an end.
“We’re definitely seeing the benefits coming through, and, again, some of the work from the PhD students suggests a lot of value to the knowledge of medical students’ and junior doctors’ about pain –and that’s something we’re now going to be able to measure.
“And it’s thanks to one of the most generous endowments of its kind in Australia, so we’re very lucky to have it here in WA.”
ED: For more details about the Churack Chair of Chronic Pain Education and Research, go to https://www.notredame.edu.au/research/ institutes-and-initiatives/churack-chair/ about-the-churack-chair.
MARCH 2024 | 13 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT COVER STORY
BACK TO CONTENTS

The little doctor who grew into his boots
The cheeriest of optimists, oncologist Dr Sanjay Mukhedkar sees the glass half full, even in the grimmest of times.
By Ara Jansen
Three Cs rule Dr Sanjay Mukhedkar’s life: cancer, cricket and cinema.
The medical oncologist was born and raised in Hyderabad, India, by two doctors who valued education. Sanjay, the elder of two boys, often joined his father on home visits and carried his kit bag.
“His patients saw him as a bit of a demi god,” says Sanjay of his father. “He was a lifesaver. Patients respected him and were grateful. The patients used to call me ‘little doctor’ so I started to think it was my destiny and the universe wanted me to be a doctor. I never entertained anything else. I grew up as a doctor.”
Sanjay was also a very talented chess player but in the 1970s no one thought it possible to make money from such a sport. His father dismissed the idea in favour of medical school, calling it a hobby not a profession. In hindsight Sanjay agrees with him.
14 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT CLOSE-UP
BACK TO CONTENTS
“I still play chess and once I hit 60 – I’m now 58 – I want to play on the senior chess circuit.” He’s also taught chess at a local high school. He studied at Hyderabad’s Osmania Medical College, gaining his qualifications as a general surgeon. His subsequent route to Perth took a somewhat circuitous path. After marrying Dr Ashwini Davray, a specialist physician in palliative medicine, in 1994, they lived and worked over the next decade in New Zealand twice, resat their qualifications, worked in New York and returned to India for a spell. During that very busy time trying to establish themselves, their eldest son lived with his grandparents in Bahrain for a year. Once settled back in New Zealand, the family were reunited, and their second son was born. Sanjay and Ashwini took turns getting their RACP qualifications while raising their sons and being away from familial support.
“I felt like that was the first major failure in my life,” he says about having to go back to study and largely start over professionally after a decade. “It was quite soul shattering and I was depressed.”
That lifted when Sanjay unexpectedly transitioned into oncology after working with a doctor in Tauranga, on the NZ north island for six months.
“I thought it would be too depressing but, instead, in those six months, I was blown away. Never had my work been so appreciated. It was something so different that I had never experienced before.
“Those last six to 12 months are a spiritual journey for the patients. Their time is limited, they know it and they thank everyone around them. It’s very beautiful and during that time a lot of people learn the art of living. It has taught me to always say thank you loudly and profusely.
“This work has had a huge influence on me. I realised I needed to use my life to help people and give back to the community. We are Hindu by faith, but service to humanity is my religion. It’s gratifying to help people.”
The Mukhedkars were considering other cities, such as Toronto, London and Edinburgh, but Sanjay was offered a job at Sir Charles Gairdner Hospital and the family

moved to Perth in 2003. The city was also closer to India in case anyone had to rush back. He started as a trainee at Charlies, in 2006 completed his training, and became a junior consultant at Fremantle Hospital, later moving to St John of God Murdoch where Sanjay has been ever since.
In 2010, he established Oncology West with Associate Professor Kynan Feeney and Dr Daphne Tsoi. It’s now the largest private group of cancer specialists in WA.
Never one to rest on his laurels, Sanjay is on the board of Cyclowest, a group committed to providing nuclear treatment to patients around the world. Sanjay is working to achieve its vision of developing modern cyclotron and GMP radiopharmaceutical facilities for Australian and Asia-Pacific markets.
Sanjay’s goal is to give smaller communities in Asian countries, particularly in rural India, access to these facilities in portable form.
In December, he was named St John of God Murdoch’s top doctor for 2023. Sanjay feels a circle was completed because his father had won a similar award from his
hospital in India at the same age.
“It took me 17 years to receive this award and I’m very grateful. It was very special for me because of the joy I could see in my wife’s and my boys’ eyes.”
While it doesn’t fit into the pithy three Cs, family is also hugely important to Sanjay. With two busy parents, Thursday is date night for the couple when they’ll usually try a new restaurant, and Tuesday night is reserved for karaoke.
Sanjay refuses to be drawn on how good a singer he is or isn’t, but insists his wife has a “lovely voice”. They also share a love for Bollywood films and take every opportunity to catch up on the latest ones.
The pair met at medical school and started dating. When they decided it was something more serious, it was time to get the blessings from their families. In a country known for its arranged marriages, Sanjay and Ashwini made a love match. Their grandparents were a little hesitant at first, but the pair eventually won them over.
MARCH 2024 | 15 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT CLOSE-UP
continued on Page 17 BACK TO CONTENTS

16 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
team
and
Stay tuned for the opening of our new clinics: Armadale North – Open April 2024 • Murdoch Square – Open Mid-2024 perthradclinic.com.au Doctor Priority Line For urgent bookings and enquiries 9599 3929
Radiological Clinic
At PRC, your referrals for musculoskeletal (MSK) investigations and pain injection procedures are locally reported and managed by the largest
of MSK
Spinal radiology experts in Perth. Our elite MSK and Spinal radiology teams specialise in providing expert imaging and pain injection services across the board, expediting treatment pathways with precise diagnostic insights. We offer MRI appointments in the evenings and on weekends for your patients’ convenience.
Experience diagnostic imaging excellence at Perth
The little doctor who grew into his boots
continued from Page 15
“We were very clear on that. We wanted everyone to bless our marriage. We believe a lot in those blessings and we have managed to be together almost 30 years and still going strong. We’re soul mates, but that’s hard work.”
Ever the proud dad, Sanjay says his sons Varun, an environmental engineer, and economics student Varad, have this wonderful ability to move between their Indian heritage and their Australian upbringing.
“I love that they can be Indian and speak to their relatives and also be with their Aussie friends having a barbecue. It gave me great pleasure that they went to India on their own last year to see the Cricket World Cup.”
Speaking of cricket, Sanjay loves to watch the game and play it, something he plans to continue doing well into his 60s. He spends

hours on the cricket pitch – he’ll happily play in 40 degrees – and founded the Australian Indian Medical Association cricket team, the AIMA Tigers. In their third year, they’re a competitive lot.
“I was playing every Saturday and as the local Indian community continued to grow, I felt it was a good way to bring people together. All on the team are doctors, we’re all crazy about cricket and don’t take defeat very well.”
He’s also starting a cricket academy where young, talented Indian
are specifically designed for those in the medical profession:
players who couldn’t otherwise afford it are able to come to Perth, play cricket and participate in skills workshops. Sanjay also plays in an over-50s team and the AIMA field a team in an indoor women’s competition.
“I never want to stop playing. A healthy mind needs a sound body. I always encourage people to play sport. I’m a big believer in it for mental and physical health. Plus, humans are social animals, we like to be with our friends. One of the biggest disasters we are dealing with at the moment is loneliness. If our needs are met, the next big thing we need is to feel wanted and loved, that’s so very important. Sport can help with that.
“Physical activity is also important for male bonding. I encourage group sport to bring people together in a team, rather than striving for individual glory. That’s like medicine – people working as a team.”

PHONE:
EMAIL:
MARCH 2024 | 17 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT Our ‘Smart’ Medical plans
– Practice Growth – Finance Structuring – Tax Planning – Cashflow Pressures – Wealth Creation – Personal Insurance – Superannuation – Estate Planning
08
6458 0644
savannah@saviwealth.com.au www.saviwealth.com.au
janean@saviwealth.com.au
CLOSE-UP BACK TO CONTENTS
Is there a doctor in the House?
GP-turned-politician Brian Walker does not mind being called unconventional and is happy to march to the beat of his own drum.
By Cathy O’Leary
FEATURE
BACK TO CONTENTS 18 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
The party leader for Legalise Cannabis WA started the year true to form – in a row with regulator Ahpra over his decision to break prescribing rules for a patient he diagnosed and treated for ADHD. Under regulations, GPs are banned from diagnosing ADHD and prescribing medication for the condition, but Dr Brian Walker says his patient was facing a one-year wait to see a psychiatrist, so he issued a script for dexamphetamine to tide him over.
The Serpentine GP and MLC knew it was against the rules but maintains he was acting in the best interests of the patient. He believes a psychiatrist disagreed, and dobbed him into the regulator.
As a result, the Member for the East Metropolitan region was hit with sanctions by the Medical Board last June, including a requirement to do an approved educational course on ADHD by the end of last year.
At the time of Medical Forum going to print, Dr Walker was doing the course but was yet to hear from Aphra whether it would accept it, given he was past the deadline.
“I really don’t care because it’s an excellent course anyway,” he said, admitting he’s not a fan of the regulator, which he claims works against the interests of the medical profession.
“The job they’re supposed to do is to keep people safe, and that’s an excellent job to have, but doctors are in fear of further action, so the actual outcomes are negative.
“I’m standing up for what I believe in, and I’m not causing any harm, so my conscience is clear. I was attempting to point out that something is causing havoc in our society and must be rectified. The principle is that we doctors need to do what’s best for our patients, not what an unelected body is telling us to do.”
Dr Walker says that in his 40-year career, he’s seen a rise in autism and ADHD.
“So, are we simply diagnosing it better or is there something happening at a societal level? These are very important questions,” he said. “I decided a long time ago that I need to stand up about these things because I cannot sit back and explain to my grandchildren that I let some things happen.”

There is a lot of greenery and leaves in his life, including at his parliamentary office in West Perth. Many naturally revolve around the cannabis leaf, a nod to the party policy that divides him from many of his medical colleagues.
Life in politics
Dr Walker will notch up three years as a politician in May – in the same year that he turns 70 – and he says his parliamentary life has been at times illuminating and surprising, and at other times disheartening. He loves being a politician, and believes it gives him more capacity to make a difference than he could as a GP only.
He is the first WA medical practitioner in the Upper House since 1971. (Dr James Hislop was elected in 1941, and retired in 1971). “And, since then, we’ve had laws come through which materially affect the medical fraternity, but no one has any experience or knowledge,” he said.
“I went into Parliament with the firm view that all politicians are untrustworthy. I had a very negative view of them, but what I’ve discovered is that most politicians are fine people, I like them a lot –they’re good-hearted, well-meaning and doing their best.
“But my view of politics as a topic hasn’t changed because one thing is evident – truth plays no part in politics, it’s about money and power.”
Dr Walker said that as leader of Legalise Cannabis WA, he had
morphed its primary policy into an approach of wellness – physical, mental, social and financial, as well as embracing social justice.
“So, when people say we’re a single-issue party, I say we’re not, you haven’t listened to my speeches in Parliament.”
But many doctors remain unconvinced by his arguments about the merits of legalising cannabis, and see him as a maverick – even a joke.
“The Government controls the narrative, and I’ve been essentially blocked from accessing the media here, and the only mention I get is when they’re trying to make fun of me,” he said. “The serious things I speak about get silenced, so people think it’s a single-issue party, because no one is reporting what I say.”
Making the headlines
Media headlines associated with him include “Pro dope campaigner says better to be stoned than drunk”, “MP asks Parliament to make cannabis available for better sex”, and his controversial Christmas card that wished people “Hempy holidays”.
Dr Walker says that while his initial move into politics was about legalising cannabis, that had become less important, and it was more about the symbolism of the cannabis leaf and its negative propaganda.
“We have status quo thinking among people who are not medically qualified. I was brought continued on Page 20
MARCH 2024 | 19 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT FEATURE
BACK
CONTENTS
TO
Is there a doctor in the House?
continued from Page 19
up with the idea that cannabis is dangerous, but it’s not, so I’ve been lied to all my clinical career,” he said.
“When we’re prescribing cannabis, I’m actually seeing two major areas of improvement, in length of life and quality of life. We’re seeing very good results, it’s a useful pharmacological tool that’s a lot safer than other options, but it’s also not for everyone.”
Dr Walker argues that the prohibition of cannabis wastes resources, and people struggling with its abuse need treatment, not sanctions.
“It’s been criminalised when we need to medicalise it. We need to offer help to these people, not prison cells. They go into prisons which become de facto psychiatric holding wards.”
He has also rubbed some doctors and health authorities up the wrong way by his scepticism on the
relative value of COVID vaccines. He is critical of some of the science cited and strongly opposed mandatory requirements at the height of the pandemic for people to be vaccinated to keep their jobs, travel or enter public places.
He says he was initially very supportive of COVID vaccines but the science behind them became a grey area.
“And when it came to the mandates, that is entirely wrong. We shouldn’t have mandates for any medical procedure,” he said. Not surprisingly, he is also strongly opposed to “no jab, no play” rules around childhood immunisation.
As far as COVID vaccines themselves are concerned, he still does not offer final judgment.
“I’m a man of science, I believe fundamentally that science shows the way, but what really upsets me is all the misinformation and disinformation,” he said. “As a result of that, when it comes to
COVID, I’m unable to decide if the vaccine has more positive or negative effects because the water is muddied on both sides, and that bothers me tremendously.”
Maternity hospital rethink
Dr Walker is similarly critical of the lack of clear evidence around the State Government’s sudden decision to change the location of the new women’s and babies’ hospital.
“There was two years of research into the location (at QEII) and a very good plan and then all of a sudden that changed within a week,” he said.
“So, we’ve now got the new hospital being moved next to Fiona Stanley Hospital, children are going to be dying, family members are going to be burdened and healthcare professionals are going to be stressed if a child dies on their watch when they might have saved them.
“Mental health is another example – we had a lot of new members praising the McGowan Government
20 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
FEATURE Deliver better mental health care for your Wheatbelt community Health professional training available now. Visit blackdoginstitute.org.au/cbh BACK TO CONTENTS
for spending on mental health. And I get up as a medical practitioner saying that I deal with it on a daily basis and at the front end we’re not seeing one cent of that money.
“There’s an epidemic of mental health disorders and the causes are not being addressed, so our population is suffering greatly. They’re tinkering with money and ideas without addressing the underlying root cause, and that is never a good idea.”
Dr Walker said that generally when he spoke in Parliament about issues such as mental health he was listened to with respect. “Because I’m actively at the frontline, and that’s one reason I must stay in my job – they don’t dare criticise me.”
When it comes to medical politics, he is not a big fan, and is not aligned to the AMA or RACGP.
“There are a lot of really excellent doctors out there, but I stopped going to medical conferences and hearing about how many patients some doctors see in a day,” he said.
“Dealing with the Medicare system, bulk-billing and 10-minute medicine – you cannot serve the patient in
that sort of time, you just can’t.
“So, the medical profession has been led into this idea of how do I make money rather than how to I serve my patients.”
On the same page
This moves into an area where Dr Walker finds some common ground even among his critics – the ailing health system and the bureaucracy overload for doctors.
“With the current health system, the costs are increasing and as a business model it must fail, so we need more doctors committed to wellness at the grassroots – more preventive medicine like watching sugar in the diet, drinking more water, exercising more, getting good sleep and good mental health, rather than relying on ‘when you get sick, here’s a pill to fix it, next patient please.”
He said that with bulk-billing, doctors were having to make sacrifices because the Government was not prepared to look after patients.
“I would like to put out a call to my colleagues to stand up and give
a voice to what the community needs, because we’re trusted by the people and we care about wellness.
“We must get our doctors properly trained and with the confidence to say this is who we are, and we can get out there and serve the population.”
He says country doctors are being demoralised so it was little wonder it was difficult to attract and retain them. Likewise, GPs were drowning in bureaucracy and paperwork.
“When you’re prescribing a Schedule 8 drug and you have to call to get authority to prescribe it, that takes up my time and the time of the patient,” he said. “It’s some sort of job creation scheme, where what you’re saying is that we don’t trust you, the doctor.
“We’re deskilling, demotivating and demoralising doctors and turning them into some sort of super-trained nurse practitioner. I would argue that we need to fight against this, we need to stand up for science and good medical ethics.”
ED: Do you agree with Dr Walker? Send us your views at editor@mforum.com.au

FEATURE
ELEVATING CARE IN THE OUTBACK Rural Health West is proudly funded by the Australian Government Department of Health and Aged Care and WA Country Health Service 16 AND 17 MARCH 2024 HYATT REGENCY PERTH n BOORLOO REGISTER NOW SCAN THE QR CODE BACK TO CONTENTS MARCH 2024 | 21 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
Aligning robots and business with surgical precision
With the Da Vinci robotic surgery unit recently celebrating its 20th anniversary in Australia, Medical Forum talks to one expert on issues preventing wider use of medical robots.
By Eric Martin

Despite being in use for decades, the development and uptake of medical robots, including the ‘holy grail’ of remote deployment to boost access in regional areas, remains untapped.
According to one of the world leaders in the field of robotic innovation in healthcare, Dr Chris Jeffery from Convergence Medical, a Queensland startup with global reach, the main hurdles are the current accounting and business models by which robots (and their crucial replacement parts) are integrated into the supply chain –blowing out costs and pushing up prices.
“Robots have existed in surgery for over 30 years. The problem with that is the business model has always been wrong and,
specifically, wrong for us here in Australia,” he said.
“Da Vinci, as of 2022, had only commercialised 8000 robots worldwide in the whole 34 years of the company. Smaller businesses do not have the budget to take on that type of investment, which pushes it out of the reach of so many people.”
Dr Jeffery knows his subject. In addition to two tours of duty as an army officer to Afghanistan and Iraq, he has an engineering degree, a medical degree, and a business degree, as well as a host of medical devices successfully commercialised on the US market including the new V01 Arthroscopic Surgical Robot, which has just been approved by the FDA.
His gift for merging medicine with robotics – and commerce – saw him awarded the Brisbane Lord Mayor's Entrepreneur of the Year in 2017, the Top 40 Under 40, among Engineers Australia’s top 10 innovators in Australia, as well as numerous other accolades.
“Robotics in Australia is probably the gold standard example of robotics in the world. But robotics everywhere has always attracted the criticism of being only 70-80% of the solution. But while robotics companies make great robots, software companies can make good software, very rarely do the two combine to create a platform that is suitable for the end user,” Dr Jeffery said.
“Robotics companies, and this includes some of the biggest ones in the world, are not structured to
22 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT FEATURE
BACK TO CONTENTS
create solutions. They are structured to create tools, a platform from which engineering companies with extensive funding and resources can then make solutions.
“Robots are a tool, but they need to be shaped for the application at hand, and, in Australia, we're as good as anywhere in the world, in fact, better than most. We currently have the capability to design enduser solutions for cardiology and radiology. You could deploy a robot to better service those markets and you could have scans done rurally, which would be amazing.
“But because of that disconnect, we do not have a lot of those end innovations, which are really the point of it all. And unfortunately, because of that layered effect, you also get bloated costs.”
Dr Jeffery believes that healthcare has not yet seen the best of what it can achieve but has always been restricted by a lack of innovation in terms of equipment.
“People always assume that medicine is at the forefront of technology, transformation and performance, and it’s true you do have to be gifted and talented to operate in that space. However, the tools, time and time again, in all aspects of orthopaedics (and I assume all other aspects of medicine as well) is where the innovation is underserviced,” he said.
“A lot of the tools we still use are basic, primitive, mechanical tools – carpenters working on a kitchen in a high-rise would have fancier things now – and, really, it has limited surgeons. Surgeons do not have enough hands, the manual tools lack the precision to get the job done, and there is a lot of cognitive distraction. The physical strain leads to fatigue, which can lead to mistakes or at least detract from perfect care.”
He said 30% of orthopaedic surgeons would admit that they were not quite confident with all of their own techniques, 70% of surgeons regularly face musculoskeletal pain, and 10% have had at least three weeks off in the past 12 months due to an occupational injury.
“Equipment breaks in one in 10 cases, and that’s in a situation where we often do between 8-12 cases in a day,” Dr Jeffery said. “And that can be higher, such as

during an ACL reconstruction where that number is closer to one in five.
“And in 40% of cases some kind of error occurs that leads to injury inside the joint, because the technology and the devices we use are limited. We are asking a lot from surgeons without really providing the proper tools they need to do it.”
By the time he began playing with the initial idea for the V01, the surgical statistics and potential solutions were worrying Dr Jeffery.
“A robot provides the solution: it's no surprise that patients do better when you can operate faster and in a more reproducible manner, trying to cause less trauma along the way, and there are no barriers to or where you can use it.
“However, the problem with medicine is that while we can make better tools, if it is not commercially viable in the face of an already strained health care system, it will not work.
“There are already so many margins in healthcare. It's not about adding to the cost, it's about moving those costs around. This was never a question for us, it was always a problem that we needed to solve: if we wanted to make a better tool, we needed to have a market that was able to benefit from it.”
Dr Jeffery said his thirst for throwing himself into projects learned during war, combined with a passion for researching and publishing that emerged almost as soon as he returned and enrolled in medicine in 2009 were his driving forces. His breakthrough moment came
when he realised that defining a robot as capital equipment, which is how arthroscopic devices and surgical robots have been commercialised in the past, was the main economic factor restricting access and a significant barrier to care.
In Australia, orthopaedics had slowly been moving to case-based billing where all the implants were transacted as consumables.
“I saw that if we can make a robotic platform that did not need to be sold, but could fit within that existing consumable model, then we could also have a business model that works. We looked at the current consumables that were not really performing and found that was enough to fund a robot,” he said.
“Capitalisation of sales has very much restricted access, and we understood that with our design. We wanted a solution where we didn't have to sell robots but, rather, consign one to hospitals or surgical centres under usage agreements – no-cost loans if it was being used and not rusting in a corner.
“And to do that, we needed to keep the costs of the robot platform low. So, we vertically integrated our manufacturing.
“Being vertically integrated means that you don't buy a robot arm, which is what a lot of robotics companies have done in the past. You build all your software and the technology from the bottom up
MARCH 2024 | 23 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT FEATURE
continued
25
on Page
BACK TO CONTENTS


Get a quote today at rac.com.au/life The RAC Life Insurance suite of products is issued by NobleOak Life Limited, AFSL 247302. Factual information only – not financial advice. Consider the PDS to see if it is right for you. PDS and TMD available via rac.com.au/life. *Offer T&Cs on site. Offer starts on 15 January 2024 and ends on 28 March 2024; applies if cover is issued. R19558 Receive one month free * when you apply for RAC Life Insurance Apply by 28 March 2024 DIRECTLIFE INSURANCE 2022 - 2023 OUTSTANDINGVALUE
Aligning robots and business
continued from Page 23
to realise maximum cost savings –we actually manufacture all these robots here in Brisbane.
“Obviously, that has a technical burden. You need the team size and infrastructure, which comes with a cost point, and then you still need the software infrastructure.
“But basically, a robot arm is a bunch of motors, computer chips and brackets and those brackets can be made pretty much anywhere.
“The computer chips are also pretty run of the mill, they can be printed at volume, and are low cost. And while integrating the motors can be a barrier, they are screaming out of the production runs in big volume.
“We start at the motor, and we build the arms ourselves. Similarly, we did not use existing companies' software, we built it all ourselves, so no licensing rights or any bloated
overheads, keeping the price low.”
The second thing he noted was that if hospitals did not own the robot, then they obviously could not be expected to pay for maintenance.
“We also needed to redesign the areas of the robot that were prone to failure to act as consumables too,” Dr Jeffery said.
“Once we saw that clarity, we had our mission, vision, and purpose –to advance arthroscopy and make surgical practice better through the introduction and use of technology. We knew what we had to do, and we knew how to do it.
“And we had a business model: removing that capital sales obligation and maintenance burden that healthcare sites currently have and replacing it with something that they already cater to – using single-use sterile consumables during the operation.
“We then bundled those
consumables, based around the things that are already used in arthroscopy, as sterile consumable devices, and that bundling allowed us to fit into the existing transactional business model of case-based billing, while providing a robot at no cost and with no maintenance overhead. That was the most important innovation.”
The final V01 robot was developed as a non-sterile reusable platform, which has nearly 20 individualuse consumables that click onto the robot at the points which are commonly prone to failure depreciation.
“This is the AI and robot era we are heading into. We have had the manufacturing era during the ascent towards the end of the century, we have had the dot-com era, and now we will see AI and robots transform everything around us,” he said. “I think medicine is just another primary aspect of that.”
Ramsay Clinic Hollywood GP referred Inpatient and Day -Patient C are for Eating Disorders
Ramsay Clinic Hollywood provides specialised inpatient and day patient services for patients struggling with eating disorders. Treatment comprises a mix of psychiatric interventions, psychological care, nutritional support and peer worker involvement.
• GP-referred (patient does not need own psychiatrist prior to admission)
• Patients are assessed prior to admission for the Day Program and admitted under the Consultant Psychiatrist, Dr Richard Clarke
• Inpatient Program Consultant Psychiatrist – Dr Leighton Chadwick
• Patients can enter the Day Program at any time
• An onsite support group is also available

Further information is available on the Ramsay Clinic Hollywood web site (see ‘For Doctors’ pages) or by contacting Wendy Henson
E: hensonw@ramsayhealth.com.au
M: 0417 404 776
Referral:

• A Best Practice template or writable pdf referral is available
• Email to: rchbookings.hph@ramsayhealth.com.au
• Phone 9346 6850 to discuss pre-admission tests that may be required
Note: Private health insurance, DVA cover or self-funding required
MARCH 2024 | 25 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT FEATURE
Scan to learn more
BACK TO CONTENTS

DNA unearths ancient health songlines
By Eric Martin
Researchers from the Centre of Health Policy at the University of Melbourne say the lack of research into the genomics of Australia’s First Nations people is having a serious impact on their health.
“Developing genomic reference data specific to Aboriginal and Torres Strait Islander people will assist in the diagnosis of genomic conditions for these populations,” Dr Philippa Dalach, from UM’s School of Population and Global Health, said. “The lack of appropriate reference data has led to delays in the diagnosis of genetic conditions and the use of suboptimal treatments.
“Harmful delays in diagnosis and adverse drug reactions due to the use of medicines that were unsafe based on a patient’s pharmacogenetic profile have been recognised among Aboriginal and Torres Strait Islander people.
“However, to date most of the published focus has been on inclusion in research, and discourse around genomic medicine has focused on future benefit rather than the more tangible and imperative benefits of ensuring Aboriginal and Torres Strait Islander people have access to the services they require now.”
For instance, Aboriginal people with cancer experience worse outcomes than other Australians for a range of complex and interrelated reasons, but these include genetic factors that could be more easily tracked within such a relatively small population.
26 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT IN THE NEWS
BACK TO CONTENTS

New Zealand geneticists have been working to trace pathogenesis within the Māori population and last year a team which included Dr Sarah Beecroft, from WA’s Harry Perkins Institute of Medical Research, found “a novel, possibly population-specific genetic configuration”, which caused the onset of a recently recognised neurodegenerative disease in all patients.
This was the first time that the disease, cerebellar ataxia with neuropathy and bilateral vestibular areflexia syndrome (CANVAS), was genetically examined in Māori and Cook Island individuals. They found no apparent phenotypic differences compared with European CANVAS patients, rather, the data identified a haplotype as responsible.
“The presence of a common disease haplotype among this cohort suggests this novel repeat expansion configuration is a founder effect, which may indicate that CANVAS will be especially prevalent in this group,” the authors concluded.
“Haplotype dating estimated the most recent common ancestor at 1430 CE supporting a single origin of the CANVAS mutation.”
measuring the frequency of mutations in the summarised (short read) data (in kilobytes) for a single nucleotide polymorphism (SNP), the most common cause of genetic variation based on a single change at a base position in the DNA, a nucleotide.
While some SNPs can influence a person’s susceptibility to a specific disease – and are the subject of research into cancer, diabetes, and heart disease – haplotypes are a set of DNA variants along a single chromosome that tend to be inherited together because of their proximity to one another.
Recombination between these variants is rare and most people would recognise their impact in hereditary polymorphisms such as blood types, compared to the gradual variations in human appearance that occur over time within a population.
Because of this, they provide researchers with more complete information, enabling them to track a specific polymorphism – including pathogenesis - back to its founding source.
secrets of the original occupation of the continent and the story of human evolution.
While their findings confirm that Papuan and Aboriginal Australian ancestors diversified from each other 25-40,000 years ago, they also suggest that all contemporary Aboriginal Australians (in their cohort) descended from a single founding population that differentiated around 10-32,000 years ago.
This has created an upper temporal limit for investigation, while identifying the uniquely indigenous haplogroups M42a, M42c, S, N13, O and P subtypes, which include potential polymorphisms related to cold tolerance and dehydration resistance, with one containing alleles that have previously been associated with thyroid hormone levels, a function related to some Aboriginal Australian’s specific adaptations to the central desert cold.
Further research to identify desertrelated natural selection revealed that the top candidate gene was KCNJ2, which has been linked to thyrotoxic periodic paralysis, a product of hyperthyroidism.
For those not familiar with genetics, genetic variation usually involves continued on Page 28
And this is where, back in Australia, the heavy lifting has already been done by geneticists working in the field of archaeology and anthropology looking to unlock the
MARCH 2024 | 27 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT IN THE NEWS
BACK TO CONTENTS
DNA unearths ancient health songlines
continued from Page 27
Geneticists also found a correlation between First Nations linguistics and genetics that remained significant when controlling for geography, “which is consistent with language differentiation after populations become isolated and lose genetic contact with one another”. This further refines the upper temporal limit to the advent of the Pama-Nyungan language family, about 4000 years ago, around the same time as the introduction of the dingo and certain stone tools. Significantly, this link with language could enable researchers to identify specific First Nations cohorts potentially impacted by pathogenesis based on speech patterns, tracing the spread of the Pama-Nyungan languages and cultural changes taking place across the continent in the mid-
Holocene, which eventually covered 90% of the Australian mainland.
An international team including scientists from Griffith University, proposed that geographically pinpointing the more than 250 distinct languages spoken by First Nations at the time of European contact – two-thirds of which belonged to the PamaNyungan family – and following the traditional movement of Aboriginal women along ‘songlines’ over dozens of generations, may reveal a genetic atlas of the development of specific polymorphisms and Indigenous health issues.
“Owing to the long history of continuous occupation, Australia’s Indigenous peoples are highly genetically distinct from nonIndigenous Australians, but should not be viewed as genetically homogenous. Many genetic variants are only found in a single community,” the authors said.
“However, to date, only three whole genome sequences have been described: one deriving from a historical tuft of hair from the Western Desert Australia and two others from cell lines with limited provenance information.”
Studies in archaeology have laid the foundation for future genomic health initiatives by increasing knowledge about the geographic distribution and phylogenetic structure of mitochondrial and Y-chromosome lineages that have survived in the contemporary descendants of Australia’s first settlers.
But more needs to be done, including broad and deep sampling to achieve a comprehensive catalogue of the genomic structural variation that exists across the country among First Nations peoples.
Transforming Dreams into Reality


State of the Art Laboratory and Advanced Technology
Our state-of-the-art laboratory is equipped with cutting-edge technology to improve your chances of achieving a successful pregnancy.
Comprehensive Fertility and Gynaecology Services

We offer a comprehensive range of fertility services, such as Ovulation induction (OI), Intrauterine insemination (IUI), In-Vitro Fertilisation (IVF), Intracytoplasmic sperm injection (ICSI), frozen embryo transfer (FET), egg freezing and sperm freezing.
Our fertility specialists also perform a wide range of fertility related surgeries to address issues like endometriosis, fibroids, uterine septum, tubal disease and caesarean scar defect.
Ethical pricing
We offer bulk billing for all Medicare eligible items. For additional services we provide transparent pricing with no hidden fees or surprise costs.
Holistic approach
We understand that the journey to parenthood can be emotionally challenging, which is why we offer ongoing emotional support and counselling services throughout the treatment process. Our compassionate team of health professionals are available to provide support with the emotional aspects of infertility and IVF, ensuring that you feel cared for every step of the way.
Video consultation
Our video consultation service is available at no extra cost for those who are unable to attend consultations physically.
Convenient locations
Oasis fertility centre has created two state of the art beautifully designed practices to best facilitate the fertility journey at South Perth and Warwick.

Dr

Dr

Dr

Dr
Phone: 1300
Email: admin@oasisfertilitycentre.com.au
oasisfertilitycentre.com.au
28 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
Santanu Baruah
Philip Rowlands
Aali
Shanaz
Chanemouga Soundaram Coundjidapadam
Fertility
Welcome to Oasis
Centre
Scan the QR code to view our Fertility Toolkit for GP’s
654 South Perth Clinic - Suite 5, 38 Meadowvale Avenue, South Perth 6151 Fax: 6182 4479 Warwick Clinic - 10/26 Dugdale Street, Warwick 6024
241
IN THE NEWS BACK TO CONTENTS
Hearing link in dementia studied
WA’s Ear Science Institute Australia is forging ahead with its ground-breaking HearCog trial into hearing loss and dementia, ultimately to see whether hearing aids can delay or halt cognitive decline.
Many studies have shown the links between hearing loss and cognitive decline, and a landmark report in The Lancet Commission for Dementia showed that hearing loss was a priority for tackling dementia. But, so far, no definitive studies have shown that treating hearing loss will change the trajectory of cognition loss.
Dr Dona Jayakody, audiologist and research lead for the cognition and hearing loss project at Ear Science, developed the trial concept in 2015 when she began researching the link between cognition and hearing loss.
By Cathy O’Leary


“My research found that hearing loss is associated with cognitive impairment and dementia, so I was interested in finding out whether this could be delayed or arrested by treating hearing loss,” she said.
“Current data suggests hearing loss accounts for 8% of the modifiable risk factors of all cases of dementia.”
HearCog is a randomised, controlled 24-month clinical trial investigating whether correcting hearing loss using hearing aids could decrease the 12-month rate of cognitive decline among older adults at risk of dementia.
About 180 older adults with hearing loss and mild cognitive impairment were recruited.
Although the research results are yet to be finalised, several findings have emerged during the
recruitment phase and as the study started.
Participants reported a significant impact from their hearing loss on loneliness, social isolation, communication challenges and quality of life. Several reported suicidal ideations at the thought of developing dementia.
Co-lead of the study, Associate Professor Andrew Ford, said some unexpected things had emerged from the study, such as participants wanting to improve their hearing health but having no one to go home to hear with or learn from. Study participants completed detailed assessments of their hearing, cognitive skills, mental and physical health, and lifestyle. They were fitted with hearing aids, with some participants waiting a year to receive theirs, as part of the randomised intervention design of the study.
They also underwent MRI and Fluoro-Deoxy-Glucose PET imaging. The results will allow researchers to gain insight into the
structural and functional changes of the brain as a result of using hearing aids.
The trial also explores the costeffectiveness of the intervention as well as the impact of hearing aids on anxiety, depression, physical health and quality of life.
Hearing loss is the second highest cause of disability in the world, affecting 1.5 billion people, with 90% of cases being age-related.
In the HearCog trial, only participants at risk of dementia were selected. Cognitive assessment suitable for the hearing impaired are being used and data logging information is being used to track the number of hours that participants use their hearing aids.
While the trial began in late 2021, the pandemic delayed its progress, with preliminary findings now expected to be published in the middle of this year.
MARCH 2024 | 29 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
IN THE NEWS
BACK TO CONTENTS
A misunderstood weight loss needs unravelling
More needs to be done to improve care for people with cancer cachexia, says Dr Vanessa Vaughan.
Cancer cachexia affects 50-80% of people, but the condition often goes unrecognised, leaving patients and even healthcare providers grappling with its elusive nature.
Often confused or conflated with the side effects of treatments such as chemotherapy, cachexia is usually associated with unintentional weight loss, loss of muscle strength and fatigue. Reduced appetite, changes to taste and nausea are common symptoms.
Unlike starvation, where feeding more calories can lead to weight regain, cancer cachexia is a complex web of factors including inflammation, changes in the way the body produces or maintains energy, and the body’s response to the presence of cancer cells — all of which contribute to muscle breakdown.
This complexity has made finding treatments difficult, with no ‘silver bullet’ in the form of a single medication. The silent progression of cachexia can be particularly insidious, reducing the effectiveness of anti-cancer treatment and the overall wellbeing and quality of life of people with cancer.
Recognising cachexia as a separate condition allows healthcare professionals to tailor interventions that aim not just to treat the cancer but also to mitigate the debilitating effects of cachexia on a person’s overall health.
While a definitive cure remains elusive, effective management strategies can significantly reduce its impact and improve patient wellbeing.
A multidisciplinary approach is proving to be a crucial component in addressing this multifaceted condition. It involves healthcare professionals such as palliative care specialists, oncologists, nurses,


dietitians, physiotherapists and mental health specialists, as well as patients themselves.
The approach usually includes four main elements:
Nutritional support
Ensuring adequate nutritional intake is a cornerstone of managing cancer cachexia.
Dietitians may work closely with patients to tailor nutrition plans that not only meet their caloric needs but also address the specific nutritional challenges posed by cancer and its treatments. Often this includes high-protein and high-calorie food. Nutritional supplements may be recommended to bridge nutritional gaps and support overall wellbeing.
Exercise programs
Physical activity has shown promise in countering muscle wasting and improving overall strength
and functionality and providing a sense of regaining control. Tailored exercise programs developed with a physiotherapist or exercise physiologist can be adapted to a patient’s capabilities and can contribute significantly to the management of cancer cachexia.
Pharmacological help
Several drugs are being investigated for their potential in mitigating cancer cachexia, though their wide use has not yet been approved in any country except Japan.
These include appetite stimulants, anti-inflammatory agents and drugs targeting specific pathways involved in muscle wasting.
Rather than curing cachexia, the focus of these drugs is more often on controlling symptoms such as nausea, lack of appetite and pain. While no single medication has emerged as a definitive solution,
30 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
GUEST COLUMN
BACK TO CONTENTS
ongoing research holds promise for future breakthroughs.
Psychosocial support
Mental health and wellbeing play a vital role in managing cancer cachexia, both for patients and those who care for them.
Doctors, nurses and mental health professionals assist patients in coping with the emotional toll of their condition, addressing anxiety, depression and the psychological impact of significant weight loss.
They may also help families and loved ones with the stress and conflict that may come up during this time. This holistic approach recognises that managing cachexia extends beyond the physical realm, encompassing mental and emotional wellbeing.
Team approach
Research has underscored the benefits of adopting a multidisciplinary and shared decision-making approach in tackling cancer cachexia. This ensures that healthcare professionals pool their expertise to tailor interventions to each patient’s unique needs.
Studies have indicated that such collaborative efforts result in improved treatment tolerance, reduced hospitalisation rates and an overall enhancement in the patient’s ability to withstand the challenges of cancer therapies.
Patients engaged in shared decision-making processes are more likely to stick with nutritional and exercise recommendations, leading to improved outcomes.
Moreover, a collaborative approach enables early identification of cachexia, allowing for timely intervention and a more effective management strategy.
Future research must focus not only on unravelling the intricate mechanisms underlying cachexia development, such as identifying biomarkers and therapeutic targets, but also on ways to make supportive cancer care accessible for people with cancer.
Clinical trials exploring novel interventions, such as pharmacological agents and targeted therapies, are vital for expanding the toolbox for cachexia management. Large-
Surgery for Heel Pain
Heel pain is a frequent problem that presents to the general practitioner. Plantar fasciitis is the most common cause of under the heel pain. Most patients will improve with non-operative treatment but not all. Surgery is a very effective form of treatment for this condition in patients with long standing refractory symptoms. Before being considered for surgery patients should undergo at least six months of non-operative treatment that includes the following (in the appropriate order):
• Rest, avoidance of activity
• NSAIDs, stretching exercise program
• Orthotics: off the shelf or custom
• Cortisone injection (one only)
• Shockwave therapy

Surgery can be open or endoscopic. The principle part of the procedure is release of the plantar fascia near its origin on the heel. Historically only the medial half was released but recent literature supports more complete release.
scale community-based studies can provide valuable insights into the prevalence and risk factors associated with cachexia, guiding the development of preventive strategies.
The future of cachexia research hinges on collaborative efforts between clinicians, researchers, patients and the broader community.
Increasing awareness, fostering a commitment to continued research and advocating for shared decision-making will contribute to more effective interventions.
By empowering patients to actively participate in their care, the gap between scientific knowledge and the human experience can be bridged, ultimately improving the lives of those affected by cancer and cachexia.
ED: Dr Vanessa Vaughan is Sub-Dean for Global Medicine at UWA’s Medical School. This article was originally published by 360info.
By Mr Peter Ammon Foot Ankle & Knee Surgery

Open surgery is performed through a 3cm incision in the proximal arch and allows not just plantar fascia release but also decompression of the tarsal tunnel and Baxters nerve which is often implicated in heel pain.
Endoscopic plantar fascia release is indicated for those without nerve compression symptoms and is done through a much smaller incision using a camera assisted cutting device much like a carpal tunnel release.
Both open and endoscopic releases are performed as day cases and require approximately two weeks on crutches. Recovery is slightly quicker for endoscopic patients as you would expect. Patients can expect an 8090% chance of a good result from surgery. Complications are rare.


MARCH 2024 | 31 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
GUEST COLUMN
St John of God Medical Centre Suite 10, 100 Murdoch Drive, Murdoch WA 6150 Telephone: (08) 6332 6300 Facsimile: (08) 6332 6301 www.murdochorthopaedic.com.au Murdoch Orthopaedic Clinic Pty Ltd ACN 064 146 774 ABN 23 070 745 210
BACK TO CONTENTS
Plantar fascia origin
GP Urology Masterclass 2024
The Westin, East Perth | Saturday 8th June 2024
Please book a place for the conference at gpurologymasterclass.com.au
Limited seats available

Dr Shane La Bianca
Dr Andrew Tan
Dr Jeff Thavaseelan
Dr Trent Barrett
Dr Matt Brown
Dr Manmeet Saluja
Dr Alarick Picardo
Dr Steve McCombie
Dr Sarah O’Neill
Live with ease.
Expert urological care and surgical management.
With the largest partnership of Urologists in Western Australia, Perth Urology Clinic can manage all urological conditions, offering a wide range of treatment options.
For urgent referrals or queries, use our GP Hotline on 1800 487 656 (Press 9). refer@perthurologyclinic.com.au
Healthlink: puclinic
Hollywood Clinic | Wexford Clinic
32 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
7 TH ANNUAL
Changing behaviours is a journey

Education is not enough when it comes helping people eat better, according to Curtin University academics Hayley Breare, Professor Barbara Mullan, Dr Chloe Maxwell-Smith and Professor Deborah Kerr.
Many Australians do not meet recommendations for common health-enhancing behaviours, such as eating fruit and vegetables, engaging in physical activity and reducing smoking and alcohol consumption – putting them at risk of poor health.
As such, the role of health professionals in primary healthcare is important for targeting risk factors of chronic health conditions and they are typically taught to educate and inform patients to prompt improvements in health behaviours.
However, for many patients, simply having knowledge about how and why to engage in health behaviours is not enough for them to want to change or allow them to have the opportunity to engage in the behaviour.
For example, while many people are aware of the Go for 2 & 5 fruit and vegetable campaigns, only one in 13 Australian adults eat enough fruit and vegetables.
Therefore, within the current healthcare landscape, it is important that effective strategies are used to support patients in changing their behaviour.
Changing mindset
One practical approach is using behaviour change techniques which provide a toolkit of strategies for health professionals supporting patients. Behaviour change
techniques have been described as the ‘active ingredients’ that make up health interventions and are commonly used across different health behaviours.
For pharmacists, this might involve the ‘restructuring the environment’ technique, where the pharmacist works with the patient to identify which cues or prompts might support them with their treatment adherence (e.g. alarm reminders, putting medication next to a toothbrush). In addition, a pharmacist might use social support. For example, providing monitored dosage systems or blister packs or facilitate the patient’s adherence to medication.
For dietitians, this might involve the ‘reframing’ technique. For example, with patients who might be disappointed with their current progress, the dietitian might be able to help them reframe from “I didn’t meet my dietary goals this week” to “I reached my goal three out of seven days this week.”
Alternatively, a dietitian might work with a patient to help them identify the ‘pros and cons’ of making the change (e.g. reducing foods high in saturated fats) or not making the change.
Tailoring intervention
There are many different techniques that can be used to change behaviour, however there is also no ‘one size fits all.’
Understanding the experiences of patients is important to tailoring the combination of techniques that may help.
Some techniques are targeted at improving capability to practise health behaviours, while others focus on overcoming barriers to opportunities (ie. time, cost, resources) and targeting motivation for healthy change.
Every little bit helps
Interventions can be as little as 30 seconds and these interactions can have a small but meaningful impact on the individual. With many health professionals seeing patients for short period of time, using one of these techniques is better than using none.
While there is great potential for the benefits of health professionals using behaviour change strategies with their patients, especially with those who find it hard to change, we’re not aiming for a workbook that will end up in a desk drawer.
What is important is that health professionals feel confident and motivated to know when and how to use behaviour change techniques in real-life situations to help their patients.
MARCH 2024 | 33 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
GUEST COLUMN BACK TO CONTENTS
Advert removed in compliance with Medicines Australia's Code of Conduct and the Therapeutic Goods Administration's Therapeutic Goods Act.
https://medicinesaustralia.com.au/code-of-conduct/about-the-code/ https://www.tga.gov.au/legislation-legislative-instruments
52 | APRIL 2021 MEDICAL FORUM | CARDIOVASCULAR HEALTH
Dr Joe

There is the adage that an economist knows the cost of everything but the value of nothing. This may be unfair to economists and is more aptly applied to politicians and bureaucrats.
The numbers tell a story
While numbers can be manipulated (lies, damn lies, and statistics), raw numbers can tell a story. On January 31, the Productivity Commission reported “…total government recurrent expenditure for health services for the latest years covered in this report was $150.9 billion.” Public hospitals cost $90 billion in 2021-22, with primary and community health a mere $55.4 billion.
In 2022, there were 38,881 GPs – 29,921 full-time equivalent (FTE), equating to 115.2 per 100,000 people – a decrease from 120.9 in 2021. In WA, the number of services per person fell to 5.8 in 2022-23 reversing a three-year upward trend and consistent with national trends.
The decrease in GP numbers will not surprise anyone except perhaps the Federal Health Minister who advised patients to “shop around” for the cheapest appointment. Most of us will look for the best holiday deal or price on a new kitchen appliance but also know that cheapest is not necessarily the best value.
There is the adage that an economist knows the cost of everything but the value of nothing. This may be unfair to economists and is more aptly applied to politicians and bureaucrats.
Laws of supply and demand make “shopping around” less viable when demand exceeds supply. The numbers of young doctors electing to go into general practice has shrunk from around 50% to 15%. There is also a demographic cliff looming as “baby boomer doctors” retire over the next decade further reducing the head count and even more potently the FTE numbers. And there is that pesky demand side demographic trend of an ageing population.
Aside advising “shopping around”, what else is the government offering? MyMedicare bears an uncanny resemblance to the defunct Healthcare Homes, which were going to “revolutionise” primary care. Nobody seems to know how it will work. Ultimately it is a form of financial risk transference whereby the financial risk of health services is transferred from the government to GPs, who will be provided a fixed amount of money to provide services versus the current open-ended system.
And surveys show that the new CPD regime gets a massive thumbs down from doctors as a tick-box waste of time – hardly adding to allure of general practice.
Milton Friedman wrote that if the government was in charge of the Sahara Desert, in five years there would be a shortage of sand. The government has been in charge of the health system for a lot longer. There is an increasing shortage of health services.
MARCH 2024 | 35 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
OPINION
Kosterich | Clinical
Editor
BACK TO CONTENTS
Hidden pandemic of post-operative morbidity and mortality: Strategies for implementing perioperative clinics
By Dr Steve Same, Anaesthetist, Perth
Surgery, an essential aspect of evidence-based medical care is not without risk. One in five patients will experience a postoperative complication, and postoperative mortality is the third leading cause of death worldwide.
A recent study published in the Lancet found that a patient’s post-surgical outcome was largely determined by their general fitness, comorbid state, and overall preparedness for surgery. Perioperative clinics can enhance patient care, improve surgical outcomes, and reduce perioperative complications.
Historically, preoperative assessments were conducted in silos by individual medical specialties, leading to fragmented care and oversights.
The need for a more unified and patient-centred approach prompted the evolution of perioperative clinics, which provide a structured and multidisciplinary approach to patient care before, during, and after elective surgery. These clinics improve patient outcomes through:
• Providing detailed risk assessments with subsequent shared decision-making on the suitability of various treatment options
• Management and optimisation of comorbidities – diabetes, heart disease, COPD and OSA, renal impairment and anaemia
• Full frailty and functional capacity assessments with physiotherapy and OT-led prehabilitation and rehabilitation sessions
• Lifestyle advice and modification – nutrition and diet, smoking cessation, alcohol minimisation weight loss advice
• Cognitive, mental, and psychological assessments with full backup psychological support
• Ongoing patient and family education and involvement in the recovery process

• Continuing management and support into the post discharge period.
The key paradigm shift in perioperative care is recognising the importance of multidisciplinary input. Surgeons, anaesthetists, nurses, allied health clinicians and other specialists collaborate to provide holistic preoperative assessments.
Public hospitals and national health services have been at the forefront in establishing multidisciplinary perioperative services. Patients at high risk of post-surgical complications undergo elective surgery in private hospitals too. Thus consultant led multidisciplinary perioperative clinics are needed for private patients.
Benefits of perioperative clinics
Improved patient outcomes: Perioperative care ensures that patients are optimally prepared for surgery, reducing the risk of complications and promoting faster recovery.
Cost savings: By addressing potential health issues before surgery, perioperative care can minimise postoperative complications, hospital length of stay, hospital readmissions, and associated healthcare costs. Investing in perioperative care contributes to the efficient use of healthcare resources by streamlining preoperative

assessments and ensuring appropriate resource allocation.
Enhanced patient experience: By providing a positive and supportive experience for patients, offering education, counselling, and coordination of care to ease the anxiety associated with surgery.
Collaborative care: A multidisciplinary approach, collaborating with primary care, surgeons, anaesthetists, and other healthcare professionals to deliver comprehensive and coordinated care.
Barriers and overcoming them
Private healthcare settings often operate under tight financial constraints, and the initial investment required for establishing perioperative clinics can be perceived as a barrier. The costs associated with staffing, technology, and infrastructure may deter institutions from embracing this model of care.
Coordinating various healthcare professionals involved in perioperative care can be challenging, especially in private settings where the structure may be less hierarchical than larger institutions. Establishing a seamless workflow and effective communication pathways is essential for the success of perioperative clinics.
Change management can be a significant hurdle in private healthcare settings where established practices may resist disruption. Physicians, surgeons, and other stakeholders may be sceptical about the benefits of perioperative clinics or perceive them as additional bureaucratic layers.
To address financial concerns, an emphasis on the long-term costeffectiveness of perioperative clinics should be conveyed. Research has consistently shown
36 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE
BACK TO CONTENTS
Key messages
One in five surgical patients experience a post operative complication
Improving surgical outcomes requires a multidisciplinary approach
Perioperative services are part of the solution.
that proactive management of preoperative risk factors leads to reduced complications, shorter hospital stays, and overall cost savings. Providing evidence of the financial benefits can help garner support from administrators and stakeholders.
Private healthcare settings can explore collaborative models for resource sharing. Pooling resources with neighbouring institutions or forming alliances with outpatient facilities can help distribute the financial burden and enhance the viability of perioperative clinics. Shared electronic health record systems and standardised protocols can facilitate seamless collaboration.
Addressing logistical challenges requires a focus on streamlined workflows and technology integration. Implementing electronic health records that enable seamless information exchange among healthcare professionals can enhance communication and coordination. Automated scheduling systems can optimise clinic workflows, ensuring efficient use of resources.
Resistance to change can be mitigated through comprehensive education and engagement initiatives targeting key stakeholders. Workshops, seminars, and peer-led discussions can address concerns, clarify misconceptions, and highlight the benefits of perioperative clinics. Involving key stakeholders in the planning and decision-making processes fosters a sense of ownership and commitment.
Recognising the diversity among private healthcare settings, medical professionals should develop tailored implementation strategies. Consideration of the specific needs, size, and structure of each institution is crucial. Flexible
PERTH HIP & KNEE CLINIC welcome Dr Paul Rebgetz to our practice
models adaptable to different practice environments enhance the likelihood of successful adoption.
Perioperative clinics have evolved into indispensable components of modern surgical care, embodying a patient-centric and collaborative approach. Through comprehensive preoperative assessments, risk stratification, and multidisciplinary collaboration, they play a vital role in optimising patient outcomes and minimising perioperative complications.
The integration of perioperative clinics into standard private practice will likely become more widespread, further emphasising the importance of a patientcentred holistic approach to the entire perioperative continuum. Future surgical care undoubtedly includes an ongoing commitment to refining and expanding the role of perioperative clinics to meet the evolving needs of patients and the healthcare system.
– References available on request
Author competing interests - nil


Paul is a locally trained surgeon who brings with him experience gained from several years of interstate and overseas fellowships, and specialises in:
Hip & Knee replacement
Robotic-assisted joint replacement
Sports knee
Foot & Ankle
Upper & Lower limb trauma
Perth Hip and Knee are a specialist practice focused on the treatment of all aspects of hip and knee pathology. From arthroscopy to complex joint replacement and revision surgery, we deliver excellence in care utilising state-of-art surgical techniques and cutting-edge technologies to achieve optimal outcomes for our patients.
We are delighted to have Paul join Perth Hip & Knee and he is a valued addition to our group of experienced hip & knee surgeons. You can contact his rooms direct at rebgetz@hipnknee.com.au or on 08 6489 1766
Perth Hip & Knee
Suite 1/1 Wexford Street Subiaco WA 6008
PHONE: 6489 1700
EMAL: admin@hipnknee.com.au
www.hipnknee.com.au
MARCH 2024 | 37 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE
BACK TO CONTENTS
Advert removed in compliance with Medicines Australia's Code of Conduct and the Therapeutic Goods Administration's Therapeutic Goods Act.
https://medicinesaustralia.com.au/code-of-conduct/about-the-code/ https://www.tga.gov.au/legislation-legislative-instruments
52 | APRIL 2021 MEDICAL FORUM | CARDIOVASCULAR HEALTH
Ten-minute consult: Recurrent abdominal pain in children
By Dr Amit Saha, Paediatric Gastroenterologist, Hollywood
Recurrent abdominal pain (RAP) is defined as at least three bouts of pain occurring over a period of at least three months, severe enough to affect daily activities. It has been reported to be prevalent in up to 25% of all children of school age with no organic cause found in the majority.
Constipation is the most frequent cause of RAP in children, with up to 60% of children reported to be affected by it at some point through their childhood.
Inflammatory bowel disease (IBD) is the most important one to exclude, and clinical features with a faecal calprotectin screen (perform only in children over age four, as the normal reference range in younger children is unknown) remains effective in this situation.
Coeliac disease remains common and has increased in recent decades. Request total IgA level with a coeliac screen. Gluten should not be excluded in diet until formal diagnosis of coeliac disease is made by a gastroenterologist.
A small proportion of children may have seronegative coeliac disease, especially in association with other autoimmune conditions, and index of suspicion should be high in these children with corroborating symptoms, despite a negative serology.
Non-coeliac gluten sensitivity (NCGS) also can be a part of this spectrum and needs to be considered as does Helicobacter pylori, especially if associated with mainly upper GI symptoms and halitosis. Breath testing for H. pylori can be unreliable especially in younger children as the protocol is difficult to follow. Request a stool antigen, which has equal sensitivity.
Eosinophilic esophagitis (causing RAP) in children is on the rise, with symptoms of difficulty swallowing and the sensation of food getting stuck behind chest. It can also present at an early age with fussy eating, often in the setting of atopy. Refer for a gastroscopy

Key messages
Assess for constipation with a detailed history, especially for faecal impaction. If in doubt, an empirical treatment trial with an osmotic laxative for a few weeks is a reasonable first step
A food diary (apps such as Bowelle or mySymptoms) is a useful exercise to try and identify specific food triggers, especially with intermittent symptoms
For older children with reflux/ regurgitation, a four-week trial of a proton pump inhibitor (PPI) can be considered prior to referral.
if suspected. Food intolerances, including transient lactose intolerance is common and a trial of excluding suspected food triggers (except gluten) is reasonable.
Finally, the spectrum of Disorders of the Gut Brain Interaction or DGBI (formally called functional abdominal pains), including functional dyspepsia, irritable bowel syndrome, abdominal migraine and functional abdominal pain (not otherwise specified) must be considered as a formal diagnosis and supportive interventions often lead to an excellent outcome in these children. For adolescents, the HEADSSS screen may be a useful tool to gather corroborative information.

Who to investigate?
Children with red flags warrant further investigations. However, it is recognised that red flags and laboratory workup do not reliably distinguish organic from nonorganic causes in children with RAP. The decision to investigate should be considered on an individual basis.
Deciding to investigate includes but is not limited to unintentional weight loss, blood in stools or nocturnal stooling, unexplained fevers, abdominal mass/ hepatospenomegaly, persistent vomiting or diarrhoea, dysphagia, extraintestinal symptoms, chronicity of symptoms (typically, if >6 months) and amount of missed school
Once we decide to investigate, the following are the high yield investigations to perform in RAP in children:
Bloods: FBC, UEC, LFTs, TFT, CRP and ESR, iron studies, Total IgA and coeliac screen
Stool: Faecal calprotectin, H. pylori stool antigen and faecal MCS + multiplex PCR
Urine analysis
Endoscopy: refer as appropriate
Genetic screening for coeliac disease has no diagnostic role but can help rule out with high certainty, if negative. Blood allergy testing is unreliable and not recommended.
Blastocystis and Dientamoeba have no known pathogenic role with 50% of children aged between 5 and 10 testing positive on stool testing. Research does not support routine metronidazole for children with chronic gastrointestinal symptoms with these organisms.
Abdominal ultrasound is rarely helpful (unless abdominal mass felt etc) and should not be routinely requested.
MARCH 2024 | 39 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE
continued on Page 40 BACK TO CONTENTS
Interventional pain management for knee osteoarthritis
By Dr Reza Feizerfan, Pain Specialist, Nedlands & Murdoch
Knee pain manifests through various aetiologies, including injuries to cartilage, ligaments, tendons, muscles, and bones, as well as inflammatory conditions such as bursitis, gout, and rheumatoid arthritis. Some of other contributing factors may include patellofemoral pain syndrome, Osgood-Schlatter disease, cancer, or referred pain from the hip joint or lumbar spine.
Among these, osteoarthritis stands out as a very common cause, exhibiting a significant increase in prevalence in Australia with a 126% rise from 1990 to 2019.
Management of symptomatic knee osteoarthritis typically commences with conservative measures such as rest, cold packs, anti-inflammatory medications, physiotherapy, assistive devices, weight loss and TENS machine. When these methods fall short of providing adequate relief, more intensive treatments, including surgical interventions and interventional pain procedures, come into consideration.
Interventional pain techniques for knee osteoarthritis encompass a range of approaches:
Intra-articular steroid injection: This outpatient procedure, facilitated by anatomical landmarks or imaging guidance (ultrasound, x-ray, CT), reduces inflammation within the joint, offering short-term

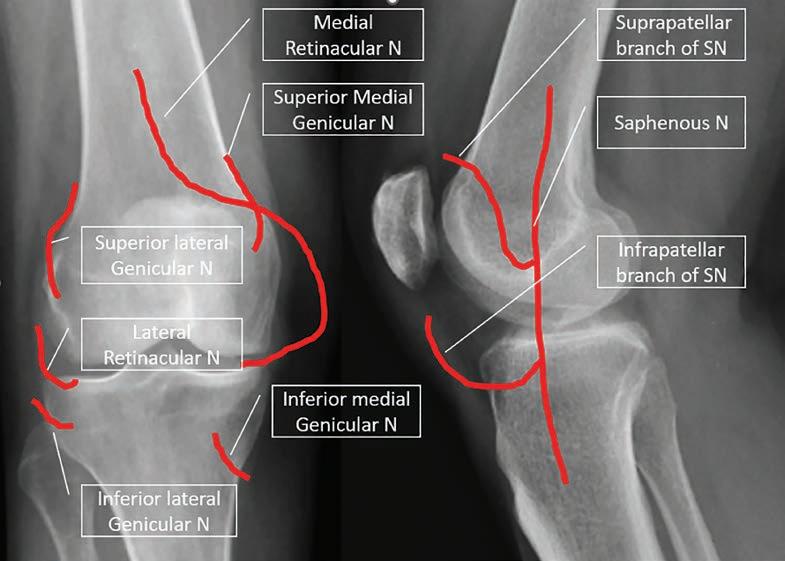
pain relief, generally for few weeks. Some of the studies demonstrated a pain reduction up to 24 weeks. The evidence suggests good pain relief with the use of intra-articular steroid injection, but only for short duration. Repeated injection of steroid may lead to cartilage volume loss; hence caution should be exercised with repeat injections.
Platelet-rich plasma (PRP) injection: PRP injections, gaining popularity in recent years, have
shown varied results in studies, with some suggesting only comparable pain reduction to placebos, while others indicate significant improvements in pain and function. In this process, the patient’s blood (around 10ml) is centrifuged. The separated plasma, which contains platelets, other cells, cytokines and growth factor, is then injected into the joint space. The theory behind it is that PRP promotes cell proliferation and
Recurrent abdominal pain in children
continued from Page 39
Treatment options:
Treatment is tailored as per cause identified. In the absence of any obvious cause, an empirical treatment for constipation is a reasonable and safe approach,
considering the possibility of occult constipation. For the DGBIs., dietary, pharmacological or psychosocial intervention can all be considered, but the overall evidence base for treatment decisions is poor.
In more recent studies, probiotics, CBT and hypnotherapy have shown
promise, but evidence regarding relative effectiveness of different strains of probiotics is currently insufficient to guide clinical practice. A multidisciplinary approach in these patients is imperative.
– References available on request Author competing interests – nil
40 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
Picture 1. Innervation of knee joint N: Nerve. SN: Saphenous nerve
CLINICAL UPDATE
BACK TO CONTENTS
Key messages
Injections for knee pain can be considered after exhausting conservative treatments
Intra-articular hyaluronic acid, steroid and PRP injections can provide a period of pain relief
Genicular rhizotomy is an advanced pain procedure that can provide a long-term pain reduction.
accelerates healing process via concentrated growth factors and proteins. Consensus about volume of the blood and frequency of the injection is still required. PRP is commonly used in knee pain from OA, meniscus and ligament injuries.
Visco-supplementation: Hyaluronic acid (HA) is a naturally occurring glycosaminoglycan and is a component of cartilage and synovial fluid. It can stimulate chondrocyte metabolism, synthesis of cartilage matrix and reduce inflammation. By injecting HA into the joint, HA aims to enhance synovial fluid viscosity, to act as a lubricant and a shock absorber.

Cochrane reviews in 2006 found HA to be effective in managing knee pain from osteoarthritis.
Genicular rhizotomy: This technique targets chronic knee pain such as osteoarthritis or persistent pain post knee replacement surgery, which are unresponsive to conservative treatments. Rhizotomy works by ablating sensory nerves around the knee joint preventing the transmission of pain signal from knee to the central nervous system. Main targeted nerves are superior medial, superior lateral and inferior medial genicular nerves. Recent studies highlighted additional nerves that can be targeted for enhanced pain relief.
In clinical practice, the selection of nerves for rhizotomy is based on patient history and examination findings. Combining X-ray with ultrasound technique can help with precise needle placement to gain a better result from this procedure. It is worth noting that rhizotomy is a technique and can be performed in different ways – thermal rhizotomy, cryo-rhizotomy, pulsed or cooled radiofrequency ablation.
While novel techniques such as

stem cell, amniotic fluid therapy and geniculate artery embolisation offer potential, further research is necessary to establish their efficacy and safety.
It's important to acknowledge the risks associated with interventional injections, including infection, bleeding, nerve injury, exacerbation of pain, and steroid side effects. Hence, while interventional pain procedures represent significant advancements in managing chronic knee pain, providing targeted relief and functional improvement for individuals with debilitating joint conditions, their application requires a balanced assessment of risks and benefits to ensure optimal patient outcomes and should be offered once the conservative managements fail to provide a satisfactory pain relief.
– References available on request
Author competing interests – nil



MARCH 2024 | 41 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE Women may book online www.breastscreen.health.wa.gov.au or phone 13 20 50 The UN International Women’s Day theme for 2024 is “Count Her In: Invest in Women. Accelerate Progress”. For over 35 years BreastScreen WA has been committed to providing a culturally safe and inclusive service to eligible participants. BreastScreen WA: • Delivers a culturally appropriate service, with resources in 32 languages.
Has 12 permanent clinics in Perth, Bunbury and Albany providing free screening mammograms.
Coordinates a fleet of mobile screening units that visit over 100 towns every 2 years across WA.
Provides after-hours appointments and online bookings.
Uses rigorous data security measures to ensure the personal information provided by clients is protected. BreastScreen WA embraces International Women’s Day 8 March 2024
•
•
•
•
BreastScreen WA_International
Day 2024 B.indd 1 15/02/2024 3:55:49 PM
Muslim Women’s Support Centre’s Pink Hijab Day, November 2023
Women's
BACK TO CONTENTS
Advancements in managing spinal pain: A comprehensive approach
By A/Prof Greg Cunningham, Spine Surgeon, Subiaco
Spinal pain poses a common challenge for medical practitioners, especially GPs in Australia, where it stands as the most prevalent musculoskeletal issue encountered by healthcare providers.
Approximately 16% of the population grapples with back problems, underscoring the need for effective and value-driven management strategies. Recent guidance from the Australian Commission on Safety and Quality in Health Care advocates for a comprehensive, multidisciplinary approach to patient care, steering away from low-value medical interventions.
It's important to note that pediatric patients with spinal pain, often having underlying pathologies, require distinct consideration and prompt investigation.
While acute low back pain usually resolves without intervention, the presence of thoracic back pain is a red flag and should raise concerns about potential sinister causes.
Considering specific anatomical causes:
Facet joint arthritis: Causes pain or stiffness, with cervical or lumbar facet pain radiating to the occiput or buttock, respectively.
Discogenic pain: Causing discomfort without muscle guarding, is often worse in the morning and may be referred to the groin from the lumbar spine.
Neuropathic pain: Nerve root compression produces typical dermatomal distributions of pain such as C6 radiculopathy to the dorsal thumb/index finger, L5 radiculopathy to the lateral calf/ great toe and S1 radiculopathy to the posterior calf /heel.
Lumbar claudication: High-grade lumbar stenosis results in lumbar claudication, characterised by pain or heaviness, limiting walking or standing.
Recent clinical care standards advocate for a selective approach to imaging, emphasising that often, no pathology is found or age-
Key messages
Spinal pain is the most prevalent musculoskeletal issue encountered by GPs, necessitating a multidisciplinary approach inclusive of physiotherapy, psychological intervention, patient education and lifestyle modifications
Specific causes of spinal pain often include facet joint arthritis, discogenic pain, neuropathic pain or radiculopathy, and lumbar claudication
Judicious use of preferably MRI imaging (including the GP rebatable cervical MRI) and accessing non-surgical interventions are valuable, while avoiding prescribing codeine is important.
related degenerative changes may induce unnecessary anxiety. In the absence of red flags, imaging is only requested after a trial of therapy.
GP referral for MRI of the cervical spine in the presence of suspected radiculopathy is MBS funded. MRI of the lumbar spine is the imaging modality of choice recommended in the clinical care standards but the lack of MBS rebate for GP requested scans is limiting.
Codeine produces hyperalgesia and allodynia and should not be prescribed to spinal pain patients. Other conventional opioids such as oxycodone have unfavourable properties. Beyond simple analgesia, atypical opioids, orphenadrine and nortriptyline are preferred.
Allied health
Physiotherapy is the typical first recommendation for managing spinal pain in the absence of red flags. In Western Australia, referral acceptance to a public hospital spinal surgery service will require prior review and treatment by a physiotherapist, aligning with practices in the Eastern States. When psychological factors (yellow

flags) are identified, active treatment is initiated to prevent chronic pain development. Referral to a clinical psychologist proves valuable for many patients, helping develop strategies to mitigate the functional impact of pain during treatment.
Multidisciplinary allied health programs (e.g. STEPS, 360 Health, and Black Swan), have been established to manage chronic spinal pain, showcasing success. Recently, in the private sector, we have coordinated a multidisciplinary allied health team aiming to model this success involving physiotherapy, clinical psychology, and a pain nurse practitioner allowing either direct GP referral or diversion of suitable patients who are otherwise waiting to see a specialist surgeon.
Non-surgical interventions
Advancements in interventional techniques have provided additional options for managing spinal pain. Under CT guidance by an interventional radiologist, most patients will tolerate (and will receive MBS funding) for one injection. For patients requiring multiple injections, typically these are better tolerated (and receive MBS funding) when performed by a pain specialist or spinal surgeon under sedation.
Epidural injections: Injection of corticosteroids into the epidural space is particularly useful for discogenic pain or symptomatic spinal stenosis.
Nerve root sleeve injections: Targeting a specific compressed nerve root provides both diagnostic and therapeutic benefits, particularly useful in an acute disc prolapse.
Facet joint injections: A source of back pain without radiculopathy, while many find these helpful, health economists do not rate these as high value care.
Rhizotomy: For patients with chronic pain originating from the facet joints. This procedure involves disrupting the nerve supply to the affected joints with a needle, providing longlasting pain relief. This procedure is usually performed under sedation.
42 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE BACK TO CONTENTS
Opioid and benzodiazepine prescribing in chronic pain
By Dr Chris Martin, Pain and Rehab Physician, Mt Lawley
The management of chronic noncancer pain (CNCP) remains a significant challenge in healthcare. While opioids are often considered for pain relief, their use requires careful consideration due to potential risks, side effects and potential harm. This article explores best practices in opioid use for CNCP, the risks associated with coprescription of benzodiazepines, and the importance of a multidisciplinary approach to pain management.
Guidelines for best practices
The use of opioids for CNCP should follow specific guidelines to ensure patient safety and effective pain management. Firstly, opioids are considered only after other nonopioid treatments have been explored and found ineffective. There is a lack of high-quality evidence to support efficacy of opioids in CNCP.
When prescribed, the lowest effective dose should be used, and the patient's pain and function regularly monitored. Dose titration should be based on clear functional benefit and risk of harm, with higher dose and longer duration of treatment considered. Appropriate time between dose titration is recommended to avoid potential risks such as sedation and respiratory depression.
Particular caution should be exercised for patients with renal impairment, liver dysfunction, elderly or patients with low body mass index. Medication selection should include partial mu-agonists, such as tramadol, tapentadol or buprenorphine as opposed to full mu-agonists, where appropriate.
Long-term preventation
Beyond providing symptomatic relief, managing spinal pain necessitates implementing longterm preventative measures.
Lifestyle modifications, including regular exercise, maintaining a
Key messages
The management of chronic noncancer pain remains a significant challenge in healthcare.
While opioids are often considered for pain relief, their use requires careful consideration due to potential risks and side effects.
Healthcare providers should screen patients for risk factors before initiating opioid therapy and consider alternative treatments for anxiety or insomnia in patients receiving opioid therapy.
Healthcare providers should also screen patients for risk factors such as a history of substance abuse, personality and mental health disorders before initiating opioid therapy. Appropriate adjustment in treatment and involvement of other specialists should be considered. Regular follow-up and reassessment are crucial to evaluate the benefits and harms of continued opioid use, consider referral to a pain specialist. Patients should also be educated about the risks, potential side effects, and safe storage and disposal of opioids.
Benzodiazepine coprescription: understanding the risks
Co-prescribing benzodiazepines, or benzodiazepine-like-medications, with opioids significantly increases the risk of adverse events, including overdose. Benzodiazepines have sedative effects like opioids, and can depress the central nervous system, leading to respiratory depression,
healthy weight, activity pacing, and ergonomic practices, play a pivotal role. Patient education is crucial in preventing recurrent episodes of spinal pain.
The management of spinal pain has evolved from outdated practices

particularly when combined. Benzodiazepines are generally not well evidenced in chronic pain management, with exception of specific conditions such as spasticity secondary to central nervous system injury/disease. Consider neurological specialist physiotherapy review if a patient presents with spasticity to ascertain degree of functional impairment and optimisation of nonpharmacological management.
Healthcare providers should exercise extreme caution and consider alternative treatments for anxiety or insomnia in patients receiving opioid therapy. Consider involvement of a psychiatrist. If co-prescription is unavoidable, it should be at the lowest possible doses and for the shortest duration, with close monitoring for signs of sedation and respiratory depression.
Multidisciplinary pain management
Effective management of CNCP often requires a multidisciplinary approach, integrating various modalities to address the physical, emotional, and psychological aspects of pain. This approach can include physical therapy, psychology (e.g. cognitivebehavioural therapy), occupational therapy, and interventional management from pain specialists. Non-pharmacological treatments such as acupuncture, biofeedback, transcutaneous electrical nerve stimulation can also be beneficial in certain patients.
This holistic approach aims to improve the patient’s overall
continued on Page 45
like bed rest and opioids. A recommended multidisciplinary approach involves allied health input, judicious imaging, and simple interventional techniques.
Author competing interests – nil
MARCH 2024 | 43 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT CLINICAL UPDATE
BACK TO CONTENTS
“One in five Australian adults are estimated to live with chronic pain.”
(Commonwealth of Australia, Department of health, 2021)
Chronic pain can be debilitating and have adverse effects on work, sleep and relationships often leading to comorbidities such as, depression, sleep disturbances and fatigue resulting in worsened health and negative societal and financial impact.
An increased reliance on pain medications and the concurrent disorders associated with chronic pain may place individuals at a higher risk of developing a substance use disorder.
Risk factors for Substance use Disorders:
Recurrent and easy access to substances
Stress and financial difficulties
Any mental illness or impairment
PTSD and trauma.
Signs & symptoms of a substance use disorder:
Frequent requests for early prescription refills
Social withdrawal or neglecting responsibilities
Physical changes; weight, poor hygiene or skin problems
Taking higher doses or more frequently than prescribed
Patient requesting prescriptions on first visit, “doctor shopping”
Changes in mood or behaviour; agitation, irritability and mood swings

Defensive or evasive when questioned about medications.
We can help...
If you suspect that a patient may have a substance use disorder, please refer them to Fresh Start, or a suitable specialist.
Referral forms can be found on our website www.freshstart.org.au or call our clinic on 08 9381 1333
44 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT E info@freshstart.org.au T 08 9381 1333 65 Townshend Road, Subiaco, WA 6008
The role of botulinum toxin type A in pain management
By Dr Jie Xiu, Pain Specialist, Applecross & West Leederville
Botulinum toxin is the most lethal substance known to humankind being 100 billion times more toxic than cyanide. It was first discovered by German physician and poet Justinus Kerner during an outbreak of botulinum in Germany due to spoiled sausages. He went on to conduct clinical experiments on himself to develop treatment and preventative measures.
The first medical use of the toxin was for the treatment of strabismus by Alan Scott in 1980. Since that time, Botulinum toxin type A is now one of the most widely used and versatile drugs in medicine, with new applications being discovered and developed.
Botulinum toxin offers a viable alternative for various types of pain management compared with existing treatments. Its analgesic effect was first noted in human studies of torticollis, where 60-80% of patients reported significant pain relief.
As of today, the only FDAapproved chronic condition that botulinum toxin can be used to treat is migraines. However, the body of evidence for use in other chronic pain conditions is growing. Research has been particularly focused on syndromes such as myofascial pelvic pain, neuropathic pain and regional pain in the shoulder, knees or back.
Key messages
Wide range of applications including headaches, nerve pain, neck and back pain
Analgesic effects beyond muscle relaxation properties
Patients who have not responded to conservative management or other treatments.
Mechanism of action
In the active state, botulinum toxin consists of a polypeptide chain with both a heavy and light chain bound by disulphide bonds. The heavy chain binds irreversibly to presynaptic cholinergic receptors at the neuromuscular junction of motor neurons, autonomic ganglia and post-ganglionic sympathetic and parasympathetic neurons.
Botulinum toxin can reduce or alleviate chronic pain through several possible mechanisms:
1. Reduction in muscle spasms and overactivity through blockade of acetylcholine release from presynaptic vesicles.
2. Reduction in neurogenic inflammation and pain. Diminishes release of neurotransmitters and peptides important in pain transmission including substance P, calcitonin gene-related peptide and bradykinin.

3. Reduction in sympathetically mediated pain through reduction in sympathetic neuron discharge
4. Reduced resting discharge of muscle spindles that contributes to reduced central sensitisation and alpha motor neuron activity.
5. Modulation of brain stem sensory neurons.
Role in pain management
Botulinum toxin is a novel agent and has a unique role in multidisciplinary pain management. It is an attractive option for patients who have failed conservative therapies and do not want many of the cognitive and addictive side effects associated with pain medications. Due to its differing mechanisms of action, it can be used in patients in whom more traditional pain treatments are not indicated or who have had a poor response to corticosteroid or radiofrequency ablation treatments. Botulinum toxin has been shown to help patients with a wide variety of pain conditions. The strongest results so far are seen with neuropathic pain syndromes such as trigeminal neuralgia and peripheral diabetic neuropathies. It should also be considered for patients with musculoskeletal pain syndromes such as chronic lower back pain, neck pain and headaches.
continued on Page 46
Opioid and benzodiazepine prescribing
continued from Page 43
quality of life, reduce reliance on medications, and address underlying factors contributing to the pain. Additionally, involving a multidisciplinary pain team can facilitate more informed decisionmaking about opioid use and help identify when it's appropriate to taper or discontinue opioid therapy.
When used, opioids should ideally be time limited and prescribed to facilitate participation in rehabilitation and physical therapies.
Managing chronic non-cancer pain with opioids requires a judicious, patient-cantered approach.
Adhering to best practice guidelines, being cautious about co-prescribing benzodiazepines, and employing a multidisciplinary strategy are
critical for safe and effective pain management. By balancing these aspects, healthcare providers can offer the most beneficial care to individuals suffering from CNCP, enhancing their quality of life while minimising potential risks associated with opioid therapy.
Author competing interests - nil
MARCH 2024 | 45 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE
BACK TO CONTENTS
Tips and tricks for common inguino-scrotal lumps and bumps in kids
By Dr Michael Collin, Paediatric Surgeon, Nedlands
Paediatric inguinal hernias are caused by the persistence of the peritoneal lining as it descends down the inguinal canal, leaving a patent processes vaginalis (PPV), which usually closes by 12 months of age. If the PPV is wide enough, it may allow intra-abdominal contents such as bowel, omentum or ovary, to descend into the inguinal canal or below, resulting in a hernia.
The child will present with an inguinal lump that feels soft and squelchy. To elicit the hernia, asking the child to strain or jump may help demonstrate the bulge if it is not initially present.
To reduce a hernia, wait until the child is relaxed and use gentle, concentric pressure with both hands and all 10 fingers. This can sometimes require a minute or so of gentle pressure. The hernia may pop out again quickly, but if it remains easily reducible it can be dealt with electively.
In boys it is important to ensure that the testis is palpable below the hernia (an undescended testis in the inguinal canal can sometimes be mistaken as an irreducible hernia). While an ultrasound can be diagnostic, its surgical use is limited to cases where there is clinical uncertainty.

Irreducible hernias require emergent review, as incarceration and strangulation can compromise both bowel and gonads. Beware overlying skin erythema, abdominal distension with bilious (green) vomiting or an unwell child.
The requirement to perform contralateral repair for the approximately 5% chance of a contralateral hernia developing should be considered against the risks. Laparoscopy or hernioscopy can assess the contralateral ring to guide this decision, and occasionally laparoscopic repair may be preferable to open repair.

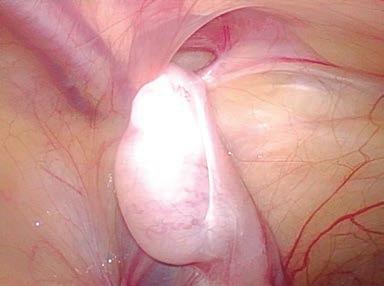
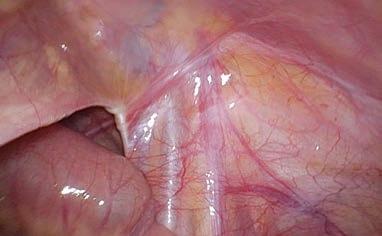
Hydrocoeles
The presence of a PPV in a male with only a small opening allows intraperitoneal fluid to drain down into the scrotum surrounding the testes and occurs in 98% of boys at
Botulinum toxin type A in pain management
continued from Page 45
Commonly, the effects of Botulinum toxin last up to three months and, depending on the pain condition, may last longer if combined with physical therapy. Overall, it is a well tolerated treatment but contraindicated in pregnancy, past hypersensitivity and neuromuscular
disorders. Other risks to consider are needle site bleeding and infection, muscle weakness and flulike symptoms.
Clinical interest in Botulinum toxin is growing rapidly. High rates of chronic pain and treatment resistance to available options on a background of the opioid crisis increases the need for innovate
treatments. In the coming years we will likely see continued research, clinical education, and recognition of Botulinum toxin in chronic pain treatment guidelines.
– References available on request
Author competing interests – no relevant disclosures
46 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE
Fig 2: Laparoscopy demonstrating an intra-abdominal undescended testis sitting near the open ring
Fig 1: Hernioscopy (a laparoscope through the inguinal hernia sac into the abdominal cavity to examine the contralateral side) demonstrating bubbles and patency of the contralateral PPV
Fig 3: A laparoscopic view of a closed internal ring with the vas coming from medial (from left of photo) and testicular vessels coming from superiorly (bottom of photo) and meeting at the ring
BACK TO CONTENTS
birth. More than 95% of cases will spontaneously resolve by one year of age and so repair should not be considered until well after then. The hydrocoele is often soft and easy to drain. Both testes should be palpated to ensure they are symmetrical.
Occasionally, a hydrocoele is tense and not drainable, or they can appear as a cystic lesion above the testes but within the cord structures (encysted hydrocoele). In these cases, or if the diagnosis is unclear, imaging with ultrasound may be appropriate. If there is any concern about underlying torsion (especially pain, tenderness or overlying erythema) then the family should be referred urgently with the child fasting to an emergency department with paediatric surgical services. A simple hydrocoele should otherwise be given the chance to resolve spontaneously with consideration for repair if it persists or reappears beyond two years of age.
Undescended testes
While 3% of boys will be born with undescended testes (UDT), a testis may continue to descend
Key messages
The diagnosis for common inguino-scrotal pathologies in children is usually made clinically
The timing and age for referral and surgical correction depends on the indication, with some conditions able to be initially observed for resolution
Beware the tender testes (either scrotal or inguinal), especially with erythema, that may be a torsion event and need urgent review and management by a surgeon.
towards the base of the scrotum until three months of age, and only one percent of all boys will go on to require repair. It is ideal to repair an UDT soon after six months of age to aid in germ cell maturation and decrease the risks of trauma, torsion and malignancy.
The most common misdiagnosis is retractile testes. All boys have a cremasteric reflex that retracts the testes superiorly when they are cold or threatened (including an examining doctor or ultrasound probe!). In most cases, the testes
can be milked down into the scrotum where they should stay without any tension (they shouldn’t spring back up like they are attached to an elastic band).
The examination involves using two hands and the pulps of all fingertips to gently sweep down over the inguinal region, one hand at a time repeatedly, from superiorlaterally towards the scrotum until the testis is felt or delivered into the scrotum (using soap or lubricant can help this technique). If a testis is quite retractile annual review is recommended as there is a 5% chance that it may ‘ascend’ and become maldescended needing repair.
An impalpable testis may be intrabdominal, or may have undergone a perinatal torsion event, and elective surgical review and intervention will likely be required.
Author competing interests – nil


MARCH 2024 | 47 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE
+61 1300 SKINSMART | www.skincancercollege.org ONLINE & FACE-TO-FACE REGISTER NOW Perth commencing - 26 April 2024 Join us in Perth Certificate of Skin Cancer Medicine course commencing in April! Develop your knowledge in primary care skin cancer medicine with this multi-award winning course. Build your confidence through flexible learning and hands-on practice. Learn vital skills in the diagnosis and treatment of skin cancer. BACK TO CONTENTS
Arthrofibrosis – a common side effect of joint surgery
By Kayley Usher PhD, Health and Biomedical Sciences, UWA
You may not have heard about arthrofibrosis but would be familiar with frozen shoulder (adhesive capsulitis), stiff knee, frozen elbow or stiff hip. These conditions are arthrofibrosis in different joints.
Despite a similar name, the pathology of arthrofibrosis, literally meaning fibrosis of a joint, is distinct from arthritis, although arthritic joints can have a degree of fibrosis that manifests as stiffness. Arthrofibrosis is a common and painful fibrotic joint disease that seriously reduces the quality of life for people of all ages and can cause permanent disability if not treated early and appropriately.
Knee arthrofibrosis is particularly disabling, causing difficulty performing normal activities (e.g. standing, walking, driving and getting in and out of chairs).
Fibrosis is a pathological state of over-healing characterised by ongoing scar tissue production, adhesions and contractions. It lies at the opposite end of the healing spectrum to diabetic ulcers (failure to heal). In joints, fibrosis can progressively invade fat pads, pouches, synovium, nerves and tendons.
Fibrosis can occur in any soft tissue, with organ fibrosis responsible for about 45% of deaths across the
Key messages
Arthrofibrosis is a common but often missed condition
Diagnosis is based on symptoms
Correct treatment improves quality of life.
industrialised world, manifesting as congestive heart failure, cirrhosis, idiopathic pulmonary fibrosis and more.
Why does fibrosis occur?
The drivers are tissue damage, hypoxia and inflammation arising from injury, surgery or infection. With many genes involved in healing, genetics influences the risk of subsequently developing fibrosis. Autoimmune diseases and metabolic disorders sometimes contribute.
The drivers cause fibroblasts (and certain other cells) to transform into myofibroblasts, the scar makers. Myofibroblasts disappear in normal healing, but with chronic inflammation become senescent and immortal. Some risk red flags include early-onset osteoarthritis and a history of surgery in the affected joint.
About 8-10% of the population will develop shoulder arthrofibrosis,
Shock over clinic closure
The lack of mental health services in WA was dealt another blow last month, with Perth’s only private mental health service south of the river put on ice.
Bethesda Clinic suspended its services, with the decision blamed on a shortage of psychiatrists and poor reimbursement from private health funds.
The 75-bed mental health clinic, located in Cockburn, was only opened in March last year, after seven years of planning, building and commissioning – and a price tag of more than $60 million.
More than 100 staff have been affected by the decision to close the clinic “for the foreseeable future.”

rising to 80-90% in diabetics. Following knee surgery or injury, approximately 10% will develop knee arthrofibrosis, although estimates vary. While shoulder arthrofibrosis often resolves after about a year, after 12 months knee arthrofibrosis rarely does.
Knee arthrofibrosis is particularly common after major surgery like TKRs or ACL reconstructions meaning that even young, active sporting people are at risk. Being healthy and fit, they are commonly advised to “push through the pain” and “work harder” in rehabilitation. Unfortunately, this highly motivated group will often take this advice and press on, worsening the damage and reinforcing the inflammatory cascade and subsequent fibrosis.
Paying careful attention to pain levels can create a window of opportunity in the first six to 12 months post insult to reverse arthrofibrosis. Research into organ fibrosis supports this.
For example, curing a liver infection early can reverse liver fibrosis. However, after the fibrotic processes are successfully halted, mature scar tissue can remain and limit range of motion (ROM) for years. This is residual fibrosis, differentiated from active arthrofibrosis by lacking
Bethesda said that despite best efforts, the service was not financially viable. The move would have no impact on operations at its specialist surgical and palliative care hospital in Claremont.
48 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE
BACK TO CONTENTS
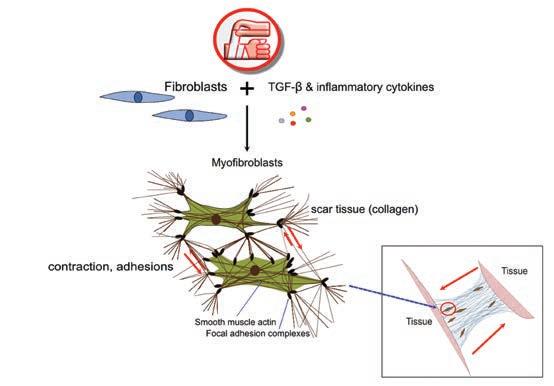
pain and inflammation. However in a joint with active arthrofibrosis swelling, redness and heat is often minimal and easily overlooked.
Investigations include tests for autoimmune and metabolic conditions and synovial fluid to rule out chronic, low-grade infection. CT and/or MRI can rule out other conditions that may cause pain and loss of ROM. Unfortunately, MRI doesn’t readily provide an arthrofibrosis diagnosis, which is based on symptoms.
Highly modified and tailored rehab is essential
for arthrofibrosis. Aggressive exercise (intensity and duration) of the affected limb is usually counterproductive and forced compliance of a joint while it’s trying to heal creates more pain, inflammation and fibrosis.
Special attention should be given to the Hoffa’s fat pad (infrapatellar fat pad), an essential immune organ. The Hoffa’s is frequently swollen in arthrofibrosis, becoming impinged and further inflamed during standing and walking. Offloading the joint using crutches for four to six weeks post-op/injury allows this to settle while regular passive stretching in the pain-free zone can increase ROM and reduce adhesions. Experienced physiotherapists recommend exercising other body parts rather than the affected limb until well down the recovery path, and then increasing use of the joint incrementally over time, as tolerated.
Aspirin (not other NSAIDs) and omega 3 fatty acids promote natural resolving pathways, and metformin and Losartan are used off label for their anti-fibrotic effects. Surgery is a last resort. Even with excellent care, the outcome is unpredictable and symptoms may worsen. Manipulation under anaesthesia – forcing ROM – risks severe complications and the immediately improved ROM is often rapidly lost.
People with arthrofibrosis need understanding and compassion. They are dealing with an invisible, painful disease that threatens their livelihoods and independence. More information is available at https://www.arthrofibrosis.info
Author competing interests- nil
WA’s first comprehensive care centre for people living with diabetes
Living Diabetes & Endocrinology is WA’s first integrated, comprehensive care centre for people living with diabetes and other endocrine and metabolic conditions delivered by a team of experienced endocrinologists and skilled allied health professionals including:
Endocrinologists
Diabetes educators
Dieticians
Exercise physiologists Podiatrists
Psychologists and other allied health professionals
Centrally located in Osborne Park with free parking, Living Diabetes is the vision of one of Perth’s most experienced diabetes specialists, Dr Joey Kaye, providing care for adult patients with all forms of diabetes including GDM, pre-diabetes and cardiometabolic dysfunction. We are also accepting referrals for all forms of general endocrine conditions.

Rapid access for new patients from March 2024 and on-going urgent referral slots
Email: admin@livingdiabetes.com.au Phone: 08 6374 6438 Learn more at www.livingdiabetes.com.au and find out more about our GP education program
MARCH 2024 | 49 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
CLINICAL UPDATE
Fig 1: An insult results in hypoxia, cell damage and inflammation. These trigger fibroblasts to transform into myofibroblasts which produce scar tissue, contractions and adhesions, and more inflammation. With chronic inflammation myofibroblasts become senescent and immortal.
BACK TO CONTENTS
When the chef met the surgeon
A chef and a surgeon walk into a kitchen. There should be a funny punchline there, but instead there is a unique collaboration that gives rise to a cookbook designed to improve surgeon dexterity.
What do a celebrated chef and an eminent heart surgeon have in common? Turns out, the kitchen.
The Heart Surgeon’s Cookbook is the brainchild of New York cardiovascular and thoracic surgeon Dr Nirav Patel MD and chef Fredrik Berselius, founder and owner of New York’s Aska restaurant and holder of two Michelin stars.
The pair accepted the challenge from the global medtech provider, Getinge, to create a unique cookbook that not only celebrates the physical and mental dexterity of both doctor and chef, but also serves as a unique training tool for heart surgeons, no matter what stage of their career.
All nine recipes, conceived and developed by Fredrik and Dr Patel include at least one surgical technique familiar to surgeons that puts dexterity to the test: precise cutting, injecting in a small, confined area, surgical
By Ara Jansen
stitching, anatomic dissecting and repetition, plus gentle handling and concentration skills. They use both surgical instruments and kitchen equipment. The doctor cooks in blue scrubs and the chef in whites.
Kartik Natarajan, Getinge’s Australian and New Zealand managing director, said surgical tools were nothing without skilled hands and the company wanted to highlight and celebrate those skills and create a challenging training tool that put dexterity to the test.
“We had seen some interesting similarities between surgery and advanced cooking, such as preparation, passion, commitment, attention to detail and the high level of precision and we wanted to explore that,” says Kartik.
With cardiovascular diseases being among the leading causes of death globally, he said we depended on the proficient hands of heart surgeons. It was hoped the cookbook would contribute to
making skilled hands even better.
Dexterity practices in the cookbook include removing the seeds from a strawberry with tweezers without harming the berry and cutting an orange wedge and stitching it back together with a needle and thread.
The food’s presentation is artful, and the recipes include sea scallop and turnip in warm broth, roasted quail with truffle, and walnut tart with caramelised ice cream. The venison and savoy cabbage features discs of cabbage filled with mushroom, folded over and sewn up with blanched chives. Some of the recipes take an hour or less, while one takes three hours to prep with a short cook time.
Apparently, the food is as tasty as the complexity and dexterity needed to make them.
“While there are parallels between surgery and high-end cooking, which is where dexterity comes in, the food is definitely worth the
LIFESTYLE BACK TO CONTENTS 50 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT


a bit of detail, step-by-step, often using images to guide even those who don’t consider themselves to be master chefs. Consider it a master class in dexterity training outside the operating room and a true challenge!”
The cookbook is available as an online flipbook or a downloadable PDF in English, Japanese, Chinese and German. Printed copies are also available.
Flipbook: https://www.getinge.com/int/ campaigns/cookbook/flipbook/
effort and tastes fantastic. Fredrik is known for his Nordic cooking and flavours, having grown up in Sweden,” says Kartik.
The collaboration for the book started early last year and took six months from start to finish. The book features a step-by-step guide to creating each dish, which the chef and surgeon created through trial and error. A series of videos also show them prepping.
Both men considered it an exciting challenge and were eager to learn from each other. The need for extraordinary dexterity is something they both have in common, although they hadn’t appreciated the extent of those similarities until they started to collaborate on the cookbook.
“Fredrik was very inspired by what Dr Patel does in the operating room. He was fascinated by the tools he uses and ways in which he could implement them in food preparation. There were many moments where he saw opportunities to bring the techniques they used back to the restaurant – such as using a scalpel or scissors instead of a knife.
“Dr Patel thought the book was a good reminder that you can always continue to learn and improve the way you move through a procedure, the techniques and sensitivity in the fingers and hands. Going forward he will encourage his students to practise using the cookbook.”
The chef has used recipes which reflect numerous ingredients from his homeland and we’re fortunate in Australia to have access to many of the high-quality ingredients he uses, including fresh fish. For those rare ingredients that aren’t available locally, the chef suggests substitutions.
The cookbook is not for the fainthearted nor the shaky of hand. While you don’t need to be a god in the kitchen to attempt it, you definitely need staying power and concentration.
“It is probably one of the most difficult cookbooks in the world, however, the authors go into quite
PDF: https://www.getinge.com/dam/ corporate/documents/marketing-sales/ brand-campaign/english/the_heart_ surgeon_s_cookbook-int-150-dpi-englobal.pdf
Physical copies to order: https://theheart-surgeons-cook-book.com/int/

WIN
Bumper movie giveaway
Everyone remembers the 1980s cult movie Ghostbusters. Now, courtesy of Sony Pictures, Medical Forum has a dozen double in-season tickets to the latest instalment – Ghostbusters: Frozen Empire, which is in cinemas from March 21.
And courtesy of Rialto Distribution, we have five in-season double passes to each of two March releases.
Cabrini tells the story of Italian immigrant Francesca Cabrini who is greeted by disease, crime and impoverished children when she arrives in New York City in 1889. She sets off on a daring mission to convince the mayor to secure housing and healthcare for society's most vulnerable.
In Io Capitano, two Senegalese teenagers embark on a journey from West Africa to Italy. This film was nominated for Best International Film at the 96th Academy Awards.
To win tickets, use the QR tab or go to mforum.com.au and hit the competitions tab.
LIFESTYLE
Scallop Turnip
BACK TO CONTENTS MARCH 2024 | 51 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
Walnut Tart
Medicine made funny

Adam Kay used to be a doctor. Now he’s a comedian who uses the stories from his time on the labour wards in the UK. He’s joining a bunch of funny people at Perth Comedy Festival in April and May.
Comedian Adam Kay says he’ll talk about anything on stage that gets a reaction – whether it’s a laugh, a squirm or a vomit.
“A particular favourite story of mine is about a degloving injury,” he says. “Hearing a thousand people gasp at exactly the same time is something that will never stop being fun for me.”
The 43-year-old British writer and comic was a doctor between 20042010, who trained in obstetrics and gynaecology before quitting to write.
“I couldn’t think of anything else,” says Adam about why he ended up in comedy. “I left medicine suddenly, after a really bad day at work and realised I didn’t actually have any transferrable skills. The only thing that vaguely approached a monetisable ability was the fact that when I was at medical school, I used to take part in various comedy sketches, so I decided to give that a whirl.”
That really bad day that caused him to leave with symptoms of PTSD was after a patient’s caesarean section was complicated by an undiagnosed case of placenta praevia. The expectant mother was taken to intensive care and the baby was delivered stillborn.
Based on his book of the same name, his show This is Going to Hurt is about Adam’s time on the UK labour wards. The stories come
By Ara Jansen
from diary entries he kept. He says while most of it leans into the silly or the disgusting, the stories don’t shy away from the harsher realities of being a doctor.
He’s appearing at this year’s Perth Comedy Festival as part of a line-up of dozens of funny people including Felicity Ward, Melanie Bracewell, Nazeem Hussain, Peter Helliar, Stephen K. Amos and former fellow doctor Jason Leong.
“I love the direct connection with an audience, something I never get through writing books or TV shows. Although, I once sat through a seven-hour flight next to someone who was reading one of my books and spent the entire-time turning the pages, stony-faced. I decided not to introduce myself.”
Since leaving medicine, Adam has done a wide variety of creative work: writing medical textbooks, founding a musical comedy group which recorded a single, writing books for children and adults as well as writing for television.
“I keep myself interested in my job by making sure I chop and change. It’s a varied diet of TV writing, performing and writing books.
“The part I enjoy the most is the feedback – I’ve had hundreds of messages from doctors all round the world saying that my stories have resonated with them or have helped
them realise they weren’t alone in struggling in their jobs. I’ve also had quite a few furious messages from parents saying that I’ve put their kids off studying medicine!”
While he’s all about the laughs on stage, Adam says he a different person in real life. His friends and family tend to find out quite major facts about him by reading his books because he finds it much easier to write things down than to actually talk to people.
“I get invited to lots of fancy parties by people who’ve seen me on stage and think I’m funny and then they’re disappointed in real life that I’m just a quiet man who stands in the corner checking his phone.”
He and television executive husband James Farrell are busy dads to Ziggy (10 months), Ruby (14 months) and a dog. When Adam does find some spare time, he likes playing the piano and watching terrible television.
One of his favourite medical quips is: “Here’s a diary entry I quite like from Christmas 2004: Full marks to the anaesthetist wearing a badge that says, ‘He sees you when you’re sleeping, he knows when you’re awake’.”
Perth Comedy Festival runs from April 22 to May 19. See www.perthcomedyfestival.com for program and tickets.
52 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
COMEDY BACK TO CONTENTS
Duke’s legacy for a new era
The Porongurups are one of our State’s great natural treasures, and planted at the foot of this ancient granite range is the Duke’s Vineyard, a part of the Great Southern Wine Region.
It was established by Duke Ranson in 1999 when his planted his first vines on his 60th birthday and has established an award-winning reputation for his wines, predominantly dry Riesling, Cabernet Sauvignon and Shiraz.
When Duke decided it was time to ease into retirement, he searched for four years to find the right person to take over, a path that led him to Ben Cane, who shares the same passion to make beautiful wines from an exceptional terroir.
This is a premium cool climate area with unique geology and has people dedicated to biodynamic viticulture, creating wines that express the philosophy of “minimal intervention” as well as respecting traditional winemaking.

Duke’s 2022 Magpie Hill Reserve Riesling
This Reserve Riesling is the perfect start to the tasting, with flinty, slate aromas bursting out of the glass with lemon zest hints. A mineral palate with lime and grapefruit, clean acid and a puckering finish. Superb is an understatement and perfect with a dozen Albany oysters.
Duke’s 2022 Magpie Hill Chardonnay
Fruit for this wine was sourced from Margaret River, the separate clones were made individually with Burgundian techniques and then blended and bottled. A light hay colour, with flinty and lemon aromas that burst onto the palate. This is still a young wine, but the flavours and textures show great potential.
WINPREMIUM WINESFROMDUKE’ S
Review
by
Dr Martin Buck

Duke’s 2021 Magpie Hill Reserve
Cool climate cabernet sauvignon is a treat in a State dominated by warmer varieties and the 2021 Magpie Hill Reserve is a stand-out wine. Restrained use of French oak hogsheads has allowed the delicate, cherry fruit to stand out among the finely structured tannins. Some complex flavours of earth and forest blend with the fruit. A very well-balanced wine with potential.

Duke’s 2021 The First Cab
This is a wine from a single clone of cabernet sauvignon planted in 1999 and with a very limited production of only 121 cases. Deep crimson in the glass and a restrained nose of berries and smokey oak. Sensational palate of smouldering fruit, forest floor and cassis. There is real power in this wine and, for me, one of the best cool-climate cabernets I have had in a long time.
Duke’s 2021 Magpie Hill
Reserve Shiraz
The Reserve Shiraz again reflects the beauty of red wines that have had minimal filtering and intervention, resulting in great textures and flavours. There are aromas and flavours of dark berries, spice and chocolate, all harnessed with silky tannins. This is a bold, muscular shiraz perfectly suited to dishes like beef bourguignon and has cellaring potential.
MARCH 2024 | 53 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
WINE REVIEW
V I N DRAYE
BACK TO CONTENTS
Ben and Duke
Heat shelters are cool

It’s been a long, hot summer and doctors want Western Australia to have more shelters to protect people during heatwaves.
Cool shelters are a way of helping to protect and offer refuge to those who don’t have access to a cool space for relief on those days when the mercury climbs past 40 degrees.
In 2021, some US cities decided to set up 'cooling centres' as historic heatwaves baked the Pacific northwest, and daytime temperatures broke records in places where many residents did not have airconditioning. Many shops had sold out of portable air conditioners, fans, water and sports drinks.
Now Australian researchers are backing the concept of cooling shelters, arguing that heatwaves are a silent killer – responsible for about 2% of deaths in Australia.
They also warn that heatwaves are set to become more frequent and intense with climate change.
WA has been suffering through a seemingly endless heatwave, with a scorching summer that has been one of the hottest on record, with prolonged spells of above-average temperatures in Perth, the Pilbara and Gascoyne.
With recent heatwave warnings in place across the State, doctors from the Climate and Health Alliance have been calling on local councils in WA and around the country to help protect the most vulnerable in their communities.
Extreme heat is one of the deadliest natural forces in this country, but more than half of deaths during heatwaves occur in the most disadvantaged parts of Australia.
Some councils have already implemented new services to protect the most vulnerable.
“Extreme heat is a killer,” says Dr Kim Loo, a Western Sydney-based GP. “We’re focused on making sure that everyone in our community has access to a cool place to go.”
Dr Loo has worked closely with council officers in the implementation of heat shelters near Blacktown where she lives and works for those most vulnerable in the community.
She is calling for other local councils to offer the same support to the elderly, people with newborn babies and other vulnerable people in the heat, as the Blacktown City Council has done.
“Extreme heat makes the whole body have to work harder,” according to Dr Arnagretta Hunter, a cardiologist at Australian National University.
“Heat can affect cognitive function, it affects our mood, our heart and our kidneys,” she said.
“Heat is dangerous for vulnerable populations, older people and very young children, but also for otherwise healthy outdoor workers for whom heatstroke can develop, causing heart and kidney failure.
“Heatwaves impact our work and also our relationships, with increased risk of domestic violence.
“It is important that potential warning signs are not ignored which may indicate heat stress, such as feeling sick, dizzy or a racing pulse, and if you encounter any of these symptoms, take action to cool down – a cool place that has fans, air-conditioning and water – and seek medical attention for ongoing symptoms.”
Curtin University expert Professor Petra Tschakert said WA’s summer scorcher had highlighted the need for urban heat action plans to protect vulnerable members of society, including facilities such as cool refuges.
“While more privileged residents simply rely on air-conditioning, many others are unable to access or afford practical ways to stay cool,” Professor Tschakert said.
“This is due to economic pressures, unfair policies and societal discrimination and puts certain people most at risk. What is needed is inclusive heat planning that takes social vulnerabilities seriously and ensures affordable heat protection for all.”
Cathy O’Leary
54 | MARCH 2024 MEDICAL FORUM | SURGERY & PAIN MANAGEMENT
IN THE NEWS BACK TO CONTENTS
FOR LEASE

DUNCRAIG
Highly Sought Rare Medical Suite
+Unique opportunity as long term tenant retiring
+98sqm medical consulting suite
+Ample parking
+3 consulting rooms
+Opposite Glengarry Hospital
Asking Rent
$34,300 pa + GST & Outgoings
For further details please contact
Rob Selid 0412 198 294

MURDOCH
Murdoch Health & Knowledge Precinct Suite 3.10, 44 Barry Marshall Parade, Murdoch
•Superbly located ‘A Grade’ suite within master-planned medical community
•195 m2 brand new tenancy
•Corner suite, abundant natural light
•2 under cover car bays
•Fit-out contribution available
•Suite may accommodate 4/5 consulting rooms, reception/waiting area, kitchen/breakout area, store records room, and other zones.
Be part of this brand-new complex and make your enquiry today.
Contact Paul Farris 0424 888 778 or paulf@rfre.com.au

HILTON
44 Victor Street, Hilton
•Well located whole building in a thriving Neighbourhood Commercial Hub
•93.2 m2* m2 lettable area
•3 consulting rooms, reception/waiting room, multiple toilets plus shower, store and tearoom
•Abundant on-site parking
•Ready for your practice now.
Contact Paul Farris 0424 888 778 or paulf@rfre.com.au
NEDLANDS
Hollywood Medical Centre
Suite 36, First Floor, 85 Monash Avenue, Nedlands
87sq m – fully fitted, large reception, 2 consulting, 2 treatment & 2 store rooms.
Contact: Irene 0409 688 339
FOR SALE

JOONDALUP PREMIUM QUALITY JOONDALUP MEDICAL SUITE – FOR SALE
•FIRST CLASS MEDICAL FITOUT
•PRIME GROUND FLOOR MEDICAL SUITE
Altegra Property Group are pleased to offer 8/189 Lakeside Drive, Joondalup to the market for sale.
This newly refurbished ground floor medical/consulting suite comprises 98sqm consulting suite+ 3 car bays, located on the corner of Lakeside Drive & Reid Promenade, within walking distance of Joondalup Health Campus with ample street parking and easily accessible public transport links.
ASKING PRICE: $630,000 + GST
Contact Anthony Morabito at Altegra Property Group on 0430 101 385 or anthony@altegraproperty.com.au
RURAL PLACEMENTS

HARVEY
Treendale Medical Group
– GP Positions
•DPA Area’s and MMM5 Available
•FSP GP’s are welcome to apply
•Busy & well established Medical Group with 4 Location in the South West of WA
•Full time & Part Time GP Positions in Treendale & Harvey
•Fully computerized and accredited modern practice with nursing and admin support
•Well supported with large team of experienced GP’s
•Situated in the beautiful South West Region surrounded by coast and forest and close to tourist areas in the south of WA
•Only 1 ½ hrs from Perth
•Family friendly working hours and no on call or hospital cover required
•65 – 70% of billings depending on experience
Please forward CV and enquiries to Kylie Wilson kyliew@harveymed.com.au
METRO PLACEMENTS

DUNCRAIG
Duncraig Medical Centre GP required
Full time patient load available.
Flexible hours seven days

LEEDERVILLE
Opportunity for a VR GP to join our busy, long established private medical practice in Leederville. Fully computerised and well equipped GP practice with Pathology onsite Our practice is fully accredited and offers full support from a well-trained and collaborative practice team. Please call Lorraine on 0487 589 829 or email practice.manager@oxfordstreetgp.com.au to discuss.
All enquiries will be kept confidential.

UNIVERSITY OF WESTERN AUSTRALIA, CRAWLEY
General Practitioner (GP) – The University of Western Australia (UWA) Medical Centre
UWA Health and Medical Services is presently seeking a VR General Practitioner (Non-DPA) to join our multidisciplinary team of health professionals. Part time or full time with no AHPRA restrictions.
About UWA Health and Medical Services
The University Medical Centre provides a range of professional, patient-focussed services in support of the University’s strategic objective to improve the quality of the student learning experience. Services are provided across a range of areas, including General Practitioner consultations; urgent medical care; immunisations; minor procedures; travel medicine; sexual health; and the management of student and staff mental health.
About the opportunity
At UWA Health and Medical Services, you’ll become part of a dedicated team of skilled and knowledgeable professionals who are deeply committed to patient well-being and contributing meaningfully to the community.
We encourage a collaborative and innovative approach to primary health care. Working alongside a team of experienced general practitioners, registered nurses, mental health nurses, administrative team and other health professionals within the wider UWA community.
What are the benefits
•Mixed Billing Practice with an attractive retention percentage
•Fully digital clinical practice
•Fully equipped and up to date treatment room
•Internal training and education to support your Medical Training and Governance requirements

CANNINGTON
PART TIME FEMALE BULK-BILLING
VR GP REQUIRED IN CANNINGTON
85% OF MEDICARE BILLINGS
OFFERED
A unique and new opportunity for a female GP to be part of a team delivering holistic women’s health care.
ESSENTIAL REQUIREMENTS
•VR General Practitioner
•Experience in antenatal / postnatal care
•Experience in contraceptive technologies
•Willing to work with interpreters
•Current Police Clearance and Working with Children Check
WHY WORK WITH US?
Ishar Multicultural Women’s Health Services is a highly reputable, not-forprofit, charity with a 30 year history of delivering specialised women’s health services to women from a refugee and migrant background.
•Flexible work hours
•85% of Medicare billings offered and no other on costs
•Brand new clinic fit out
•Experienced reception and administrative team
•Focus on a niche area of women’s health
•Work as part of a dynamic multidisciplinary team, comprising of a midwife, practice nurse, dietitian, psychologist, social worker and counsellor.
This is a unique opportunity for the right person, if you are interested in finding out more about the role please contact: Kim Duong, Services Delivery Manager; Phone: 9345 5335 or Email: kim@ishar.org.au

SUBIACO
We are looking for experience GPs with a passion to make a difference for people seeking help for substance use disorders to join our team at Fresh Start Clinic in Subiaco.
Fresh Start Clinic is the entry point for all clients and patients at Fresh Start. Our doctor’s perform general health checks, and create informed care plans for patient’s recovery.
•Fully bulk billed clinic
•Onsite Pathology
•Best Practice Software
•Nursing support
•Encourage special interest of addiction
•Immediate start
Contact Andrew, classifieds@mforum.com.au or phone 9203 5222 to place your classified advert
Excellent remuneration –$200 to $300 per hour.
Predominantly private billing practice
Modern fully computerised practice (Best Practice)
Please contact Michael on 0403 927 934 or michael@duncraigmedicalcentre.com.au
•Flexible working hours
•Excellent work-life balance
To learn more about this opportunity, please contact Sharon Almeida on (08) 6488 2118 or at sharon.almeida@uwa.edu.au
This position is only open to applicants with relevant rights to work in Australia.
•Free parking
Business hours 9am – 5pm
Monday to Friday
For a confidential discussion please email Jeff Claughton ceo@freshstart.org.au
medical forum CLASSIFIEDS 81 NEXT DEADLINE: For Classifieds, contact Andrew Bowyer – Tel 9203 5222 or classifieds@mforum.com.au

JOONDALUP
The Best GP Job in Perth – Hands Down!
Here’s a job where you finally get Treated (and Paid!) like a Specialist. We are looking for a motivated GP in Skin Cancer Medicine.
Join a clinic that puts you first and helps you excel in your career :
•100% Private Billed Skin Checks. No exceptions.
•Procedures privately billed with high gaps
•State of the art Mole Scanning Technology
•Fast on boarding, training and mentoring
•Happy staff and expert colleagues
•Expand to Cosmetic medicine or Vein Sclerotherapy
•$200 ph min
•And more…..
What are you waiting for?
moleclinic.link/Best-Job
Please contact Practice Manager on 08 9301 1825

KALAMUNDA/ HIGH WYCOMBE
•Well established and regarded medical practice, about to celebrate 60th year, offers a unique opportunity for a VR General Practitioner
•Long history of being a training practice, both GP Registrars and Medical Students.
•Main surgery in Kalamunda, with a further two surgeries in High Wycombe and second satellite surgery in Kalamunda
•Mixed billing (or private billing if preferred)
•Well organized for Chronic Disease Management and Care of the Elderly, with Primary Care (CDM) Nursing Staff at all four surgeries
•Very nurturing practice, empathic to patients and staff. Supportive of clinical team members with individual special interests (such as cosmetic and skin lesion skills, mental health, LGBTIQA+…)
•Excellent schools in the fantastic Perth Hills area, very welcoming community
•Work life balance a major priority that is respected by the team at Stirk
•Have the best of both worlds; country living with the city only 30 minutes away
Please forward a CV and any enquiries to either Karin Tatnell (0438 211 240) or Dr Mike Civil (0419 965 377 ) or email : manager@stirkmedicalgroup.com
HIGH WYCOMBE
VR GP POSITION – Full time/Part time
•A busy, well equipped, fully computerized and AGPAL Accredited GP Practice in Perth, WA is looking for a VR Doctor
•Flexible days and hours tailored to your need
•Excellent RN and reception team as well as managerial support and onsite pathology
•Clinical full autonomy guaranteed
•Mixed Billings, using Best Practice Software
•GP private ownership
•Good income potential and emuneration at 72%, negotiable.
•$150 hourly minimum for the first three months.
The practice provides general GP services including skin check and many more.
For enquiries,
Email: highwycombemc@bigpond.com
Phone: 08 9454 6987

ATWELL
Require VR GP’s Unrestricted for Part-time Positions:
As an experienced GP, this role will allow you to provide high quality primary health care services to the community, in keeping with best practice standards.
Essentials:
•Applied knowledge, skills and experience in general practice
•Unrestricted VR GP qualification
•Full Australian Work Rights
What’s in it for you:
•Supportive and Experienced Admin team
•Doctor owned practice
•Nurse Support
•Onsite Pathology
•Flexible arrangements
•AGPAL Accredited Practice
•Located near FSH and SJOG Murdoch
•Mixed Billing (mainly Private)
If you are interested please contact our Practice Manager for further information on 9332 5556 or email: adminmetrogp@metrogp.com.au
BULL CREEK
Bull Creek Medical – VR GP opportunity
We are seeking full time or part time VR GP to join our friendly team.
It is a mixed billing well established practice providing quality health care for many years.
It is located closer to world class public and private hospitals and near by top public and private schools. Flexible working hours and terms and conditions are negotiable.
If you are interested in this exciting opportunity, contact practice manager via email:
admin_pm@bullcreekmedical.com or call on 08 9332 0488
COMO

Opening for VR GP - F/time or P/time
Full Private List available now from retiring GPs
FRACGP essential
Up to 70% private billings
Unique opportunity to join our family orientated practice in one of Perth’s fastest-growing suburbs. Enjoy working for a doctor-owned, non-corporate, well supported, and accredited practice.
Please contact the Practice Manager on 6165 2444 or email: reception@comogp.com.au

GREENWOOD
Kingsley Family Practice
We are seeking a part time or full time GP to join our well established, busy practice.
You will work in a highly equipped AGPAL accredited practice, alongside GPs with extensive specialised skills, including skin cancer surgery (including flaps and grafts), cosmetic medicine, ultrasoundguided musculoskeletal PRP injections, IUD insertion, ENT operating microscope use, and much more.
The practice itself is highly equipped, including on-site ECG, spirometry, ABI machine, ultrasound, digital dermoscopy imaging, ambulatory BP monitoring and a full time chronic disease management nurse.
Mixed billing, offering our GPs 70%. All appointments privately billed on Saturdays.
For more information please email kingsleypractice@gmail.com or call our Practice Manager Tracy Weare on (08) 9342 0471

NEDLANDS
Niche, Boutique Medical Centre
looking for a VR GP Fully Private
Our practice is situated in the Golden Triangle in the Western Suburbs.
Standard consult 23 - $100, 36 - $180 We are looking for a committed GP with excellent time management.
Full-time practice nurse with outstanding administration support.
One Saturday per month (AM only) with higher rates.
Please send through your EOI to: manager@nedlandsmedicalcentre.com.au
BURSWOOD/CLAREMONT
75% OF BILLINGS!!
GP positions available in accredited mixed-billing clinics in Burswood and Claremont.
Looking for VR GPs and non-VR GP’s on a full time/part-time basis for weekday and Saturday afternoon sessions. Fully computerised with on-site pathology and RN support.
Please contact Dr Ang on 9472 9306 or Email: info@thewalkingp.com.au

Reporting to the Clinical Lead – Primary Health Care, we are currently seeking a General Practitioner, to provide service delivery to the RFDS WO traditional GP clinics including the provision of comprehensive routine and emergency general practice care to patients in remote communities and nursing posts. This is a permanent part time 0.8 FTE residential position based in Port Hedland and we would consider a job-share arrangement. The RFDS WO provides partially subsidised housing and vehicle as part of living in the community. Please contact peopleandculture@rfdswa.com.au for more information.

MOUNT LAWLEY
VR GP - Mount Lawley WA - Privately billed After Hours practice
GP After Hours Mount Lawley is a well-established, community-based after-hours practice. We privately bill and are GP owned and run.
We are looking for an experienced VR GP to join our team of clinicians in providing quality after hours care to our patients.
Our practice offers:
FREMANTLE
P/T GP required for our friendly practice in the heart of Fremantle. Young demographic with lots of student health, sexual health, women’s health and mental health. Fully equipped, accredited practice with full time practice nurse and onsite pathology, 2-3 days/week, days negotiable.
Contact Stephen on 0411 223 120 or at stephen@westendmed.com.au
•Modern facilities with a fully equipped treatment room
•Fully computerised practice using Best Practice software
•Percentage of the billings with a minimum hourly rate guarantee
•All sessions are 4 hours in duration
•Opportunity for weekend / public holiday sessions
For all enquiries, please email Gina at gpahmtlawley@3rdave.com.au or call 0412760871
medical forum CLASSIFIEDS 82 NEXT DEADLINE: For Classifieds, contact Andrew Bowyer – Tel 9203 5222 or classifieds@mforum.com.au
Contact Andrew, classifieds@mforum.com.au or phone 9203 5222 to place your classified advert
Contact Andrew, classifieds@mforum.com.au or phone 9203 5222 to place your classified advert
Join our team at Bullsbrook Medical Centre where you will enjoy every aspect of general practice. We are a well-established clinic with a strong and loyal patient base.
• Value driven, innovative, non-corporate GP owned medical centre with a highly competent administrative and nursing team, supporting the practice and allowing you to focus on servicing the patient demand.
• Large patient base with broad demographics.
• Team of GPs providing high quality care with a strong focus on comprehensive chronic disease management
• Fantastic opportunity for GP’s with special interests
• Friendly working environment of mutual support
• On-site Practice Manager, pathology and allied health.
• Fully computerised (Best Practice).
• AGPAL accredited.
• Training Practice for GP Registrars.
• Independent Contractor Agreement with high income potential
• Incentivised opportunity for FRACGPs interested in providing supervision to training GP’s.
Requirements:
Unrestricted AHPRA registration, VR/FRACGP
For a confidential discussion please contact Dr Raf Francikiewicz on 0424436663 or email raf@bullsbrookmedicalcentre.com.au

Northbridge Medical Centre is looking for a VR General Practitioner to join our well-established private billing medical practice located between Perth CBD and Mt Lawley
Owned and operated by doctors
High patient load
Taking over existing patient base from relocating GPs
Full Time or Part Time Position available now 65% billings with minimum of $150/ hour for the first 6 months
Joining a team of 6 Doctors with supportive Nursing, Management and Marketing team
AGPAL accredited, well equipped and fully computerized with Best Practice software
Doctor’s parking available
Requirement: MBBS or equivalent, Vocational Registration / Fellowship, current AHPRA registration
If you are looking to practice quality medicine in a supportive environment, please contact Dr Alex Koh on 0408 037 290 for a confidential conversation or email at Alex@northbridgemedical.com.au
Positions - Stress Test Supervising Physician
Perth and suburbs
Park Centre, East Victoria Park
Victoria Park Central, Victoria Park Waterford Plaza, Karawara New

Are you seeking a workplace focused on best practice and excellence in clinical care?
At Perth Cardiovascular Institute we believe in providing more than just a diagnostic imaging service. Our team are committed to delivering an excellent patient experience along with clinically robust findings in a timely manner.
Senior staff perform as leaders and assist with training, mentoring and development of less experienced team members. Much of our time is dedicated to ensure our trainees develop superior skillsets to tackle even the most difficult of cases. We foster an environment that promotes asking questions, seeking feedback and sharing of knowledge.
We have world class, internationally renowned cardiologists within our group that support and develop individuals. Our cardiologists are approachable to discuss patient findings and encourage and enable team members to manage patients. In completing our daily duties we go above and beyond expectation with clients repeatedly providing outstanding feedback from their contact with us.
If you wish to know more about the role, feel aligned to the way we do things and are excited by the unique opportunity Perth Cardio offers then we would be thrilled to hear from you.
Please contact Adam Lunghi on Phone (08) 6314 6881 or info@perthcardio.com.au



medical forum CLASSIFIEDS 83 NEXT DEADLINE: For Classifieds, contact Andrew Bowyer – Tel 9203 5222 or classifieds@mforum.com.au
patients welcome practicemanager@parkmedicalgroup.com.au Positions available for suitably qualified Doctors and Nurses To apply please contact: www.parkmedicalgroup.com.au ParkCentre,U2,779AlbanyHighway,EastVictoriaPark VictoriaParkCentral,U24,366AlbanyHighway,VictoriaPark WaterfordPlaza,230ManningRoad,Karawara orbookviaoron-linevia Call ☎ 9452 9999 To book your appointment

Gosnells Healthcare Centre has a great opportunity for General Practitioner to join a very well-established practice.
The role would suit a new Fellow or GP who wants to curate their own patient base with a guaranteed minimum offered for 6 months.
Wonderful, friendly practice
Experienced Doctors
Very Large existing and loyal patient base
Mixed billing practice
Enjoy an innovative, modern practice with the latest equipment and software (Best Practice)
70% of billings- plus attractive relocation package
Choose your hours, Our Clinic is open from 8am-5pm Monday-Friday.
On-site services include Pathology, Physiotherapy, Podiatry, Dietician
Fully Accredited practice
DPA Replacement Provider Number available Safety Net of $150 per hour for 6 months
If you are interested in the exciting opportunity please contact Phil at ceo@spectrumhealth.net.au
Gosnells HealthCare Centre
2227A Albany Highway, Gosnells WA 6110
We are a team of 10 doctors with excellent administrative and nursing support staff. We have been in Hillarys for 20 years with dedicated GP owners. We pride ourselves with providing exceptional health care to our community of Hillarys.
We have a modern purpose built well equipped 3 bed treatment room and 10 consulting rooms with quality equipment as well as a spacious staff & meeting room. We are also able to offer secure remote access and secure onsite parking. Pathology & Pharmacy are within our complex.
There is a high-income potential as we are mainly a private billing practice. We would also encourage doctors to develop their own special interests
Our patient base is varied as well as a strong family base practice including women’s & mens health, skin cancer medicine, iron infusions, aviation medicine and more. Our nurses are committed to support for care plans & health assessments.
We are a 7 day a week (Mon to Thur 8am to 7pm, Fri 8am to 6pm, weekends 8.30 to 12.30pm) we have a variety of sessions available and the opportunity to share a Saturday roster with your fellow GP colleagues, with nursing support.
We would require:
Current unrestricted registration with AHPRA as a general practitioner
Current medical indemnity insurance
Full Australian working rights and No DPA restrictions
For confidential discussion please phone
Dr Rod Parker 0447 117 013 or Dr William Thong 0403 171 061 or by emailing admin@hillarysmc.com
Director of Public Health & Medicine
Position will be located on Christmas Island (Indian Ocean Territories)
Full time Ongoing Vacancy | Generous remuneration package - negotiable

The Indian Ocean Territories Administration (IOTA) is currently seeking a motivated, professional and suitably qualified person to join our team as the Director of Public Health & Medicine (DPHM) within the Indian Ocean Territories Health Ser vice (IOTHS) based on Christmas Island. This position is a similar level to a Western Australian Country Health Ser vice Senior Medical Officer position.
Package valued in excess of $440,000 including:
Base salary
Employer contribution to superannuation
Commuted allowance calculated at 30% of the annual base salary
District Allowance payable in addition to base salary
Professional development expenses allowance
Generous leave entitlements
Annual return airfares assistance to Perth
Remote support package (including access to subsidised housing and vehicle) for eligible candidates
The IOTHS delivers a primary and acute health care service in two of Australia’s most remote and most spectacular settings - Christmas Island (CI) and the Cocos (Keeling) Islands (CKI). IOTHS includes a 24 hour eight bed hospital and primary care facility on CI and clinics on Home and West Islands in the CKI. The IOTHS is committed to “Working with our communities to keep us healthy for the whole of our lives”.
The DPHM is primarily responsible for the delivery of quality medical and emergency services to the communities of CI and the CKI. The DPHM will:
Supervise and support the District Medical Officers on both CI and CKI; the Medical Scientist and Community Social Worker on CI, using performance agreements and structured performance appraisals; Undertake clinical duties by providing direct patient care to the community in primary, secondary, emergency and community health care settings; Provide advice on the appropriate visiting specialist’s arrangements (medical and allied health) and for reviewing services provided;
Provide leadership to direct reports and ensure responsible, efficient and effective management of the human, physical, financial and systems resources for medical services;
In addition, the DPHM further plays a key role within the Executive Management Team of the IOTHS.
Our ideal candidate will have a demonstrated ability to lead and manage a clinical portfolio, have recent (within the last 12 months) and substantial experience working effectively in a rural or remote cross cultural environment within an Emergency Department, as well as experience in in-patient management, public health, women’s health, child health and chronic disease management. Further the successful candidate will also possess emergency life support skills and be committed to ongoing medical self education and the education of other staff.
The successful candidate will be registered as, or be eligible for, a medical practitioner with the Australian Health Practitioner Regulation Agency (APHRA), and hold a post graduate qualification and/or have recognised current clinical experience in General Practice. Further, the successful applicant will also hold a current Western Australian Working with Children Check, hold a ‘C’ class manual Driver’s Licence transferable to the Indian Ocean Territories and be subject to a health assessment and preemployment screening.
For an application pack outlining how you can apply for this oppor tunit y, please contact the IOTA Human Resources Team at IOTHRTeam@infrastructure.gov.au and quote position number 109097
Applications close 4.00PM (Christmas Island local time), Thursday 29 February 2024
medical forum CLASSIFIEDS 84 NEXT DEADLINE: For Classifieds, contact Andrew Bowyer – Tel 9203 5222 or classifieds@mforum.com.au
Hillarys Medical Centre is a very busy practice located 15mins from the Per th CBD along the coast. We have a strong focus on family & preventive health medicine
Spectrum Health knows Medical Recruitment


Spectrum Health has a team of professional and skilled managers with many years of industry experience who ensure the seamless and successful operation of medical practices. Dr Vishnu Gopalan, the Chairman of Spectrum Health helms an expansive network of medical centres with a Our GPs can expect to receive:
Attractive and rare DPA replacement provider number
Cutting edge technology using an App which increases ethical billing
High billing and good patient load
Medicare audit prevention tools
Management support
Friendly atmosphere strong intent to build genuine partnership with General Practitioners. The Spectrum Health team welcomes the opportunity to partner with you in general practice. Gosnells Healthcare Centre Calling all GPs! Empower your medical expertise and join us to make a difference in healthcare. SPECTRUM HEALTH Spectrum Health 33/9 Vision Street, Wangara WA 6065 T: (08) 9301 1015 E: ceo@spectrumhealth.com.au Website: spectrumhealth.com.au
1.
4.
2.
5.
3.
6.






Foraconfidentialdiscussionabout yournextcareermove,call Jeanat 0400605529 oremail jean.paradise@breckenhealth.com.au FRACGPpreferred,flexiblearrangements Relocationassistanceoffered Largeanddiversepatientbase,mixedbilling Yourownspaciousroom FullycomputerisedandDoctorowned Nooncallorafterhours Anamazinglifestyle opportunityforGPs Ourbeachsidepracticein Albanyis lookingfornewGPs
