








Canadian first: Thyroid nodule removal Page 5 Inside: From the CEO’s Desk | Long-term Care | Special Focus: Paediatrics www.hospitalnews.com August 2023 Edition FEATURED Are You Protected From An Unexpected Loss of Income? Our Signature package (Life, LTD and ADD&D) is tailor-made for those who already have health benefits through a spouse or other group plan. Ask us about our BONUS $1000 LTD offer when you call! 1-866-768-1477 | www.healthcareproviders.ca
PRIVATIZATION:



Nurses and health-care professionals know that privatization is a big risk. A government that truly prioritized equal access to care would be funding the public system adequately, not selling it out.



KNOW THE FACTS:


NursesTalkTruth.ca


Doug Ford is gambling with your access to care.




Contents COLUMNS Guest editorial ................. 4 In brief .............................. 6 Long-term care 26 From the CEO’s desk 28 August 2023 Edition IN THIS ISSUE: s Special Focus; Paediatrics 16 s Cover story: First-in-Canada procedure seeks to remove thyroid nodules with reduced side effects 5 s Bearing witness: The power of presence 14 s ALS diagnosis transforms storyteller into advocate 10 s Offload Specialists bridging the gap between prehospital and hospital care 29 New study finds subgroups of kids with similar brain patterns do not share diagnostic labels 18
Why is being a patient a difficult pill to swallow?
By Harvey Max Chochinov
While being treated for an aggressive hematologic cancer, the former Head of a Department of Medicine at a large teaching hospital told me he wished he could hang a sign on his headboard, reading P-I-P: Previously-Important-Person. Despite extraordinary achievements, skills, credentials, and status, being a patient made him feel like an amalgam of parts; limbs, bodily fluids, organs, and orifices, all now suspect, some more wayward than others – and most, for his taste, far too readily on display. Why is being a patient such a difficult pill to swallow?
Besides whatever concern or ailment brings you to seek medical care, there is something about the very nature of being a patient that deeply rankles. Whether trying to arrange a medical appointment, waiting to be seen in a clinic or hospital, or being examined under the watchful gaze of a healthcare provider, being a patient disrupts our sense of intactness, gnawing away like an existential termite.
At its core is the erosion of personhood and a feeling that identity is under attack, threatening to displace the essence of who we really are.
It doesn’t have to be this way.
Our sense of who we are as people is highly individualized, based on personal experiences and relationships; affiliations, attitudes, culture, beliefs, abilities; opportunities and connections; inclinations and foibles. In other words, who you are as a person is highly specific and unique; never has there been, nor ever again, will there
UPCOMING DEADLINES
SEPTEMBER 2023 ISSUE
EDITORIAL: August 10
ADVERTISING:
Display – August 25 | Material – August 29
Monthly Focus:
Emergency Services/Critical Care/Trauma/
Emergency/Online Education: Innovations in emergency and trauma delivery systems. Emergency preparedness issues facing hospitals and how they are addressing them. Advances in critical care medicine.
+ ONLINE EDUCATION SUPPLEMENT + SPECIAL
FOCUS: EMERGENCY ROOM
be one exactly like you. Being a patient, on the other hand, is based entirely on things that are generic.
Bodily parts are supposed to behave in exact and predicable ways, irrespective of who their owner happens to be. With all due respect, whether prince(cess) or pauper, poet or pilot, your bits and bobs are pretty much identical, in form and function, relative to everyone else’s.
And herein lies the problem with being a patient. The moment we enter the healthcare system, the focus of attention shifts from who we are, to the ailment or problem we are now facing. This shift puts identity in jeopardy.
A long-time dialysis nurse once told me she eventually came to think of patients as kidneys on legs. Patienthood eclipses personhood, casting a shadow that undermines the essence of who we are. This is bad for patients and their families; it is also bad for healthcare providers since emotional disconnection and objectification of patients is a harbinger for professional burnout.
One approach designed to decrease this kind of existential trauma is beginning to take hold, coined the Patient Dignity Question (PDQ). The PDQ asks patients, “What do I need to know about you as a person to take the best care of you possible”? This question forms the basis of a brief five-to-ten-minute conversation, focused on personhood. What matters to you? What are your core beliefs? What or who are you most worried about? What roles and relationships matter most?
Continued on page 6
OCTOBER 2023 ISSUE
EDITORIAL: Sept. 7
ADVERTISING:
Display – Sept. 22 | Material – Sept. 26
Monthly Focus:
Mental Health and Addiction/Patient Safety/ Research/Infection control: New treatment approaches to mental health and addiction. Developments in patient-safety practices. An overview of current research initiatives. Developments in the prevention and treatment of drug-resistant bacteria and control of infectious (rare) diseases. Programs implemented to reduce hospital acquired infections (HAIs).
+ANNUAL INFECTION CONTROL SUPPLEMENT
THANKS TO OUR ADVERTISERS Hospital News is provided at no cost in hospitals. When you visit our advertisers, please mention you saw their ads in Hospital News.
610 Applewood Crescent, Suite 401 Vaughan Ontario L4K 0E3 TEL. 905.532.2600|FAX 1.888.546.6189 www.hospitalnews.com
Editor Kristie Jones editor@hospitalnews.com
Advertising Representatives
Denise Hodgson denise@hospitalnews.com
Publisher Stefan Dreesen stefan@hospitalnews.com
Accounting Inquiries accountingteam@mediaclassified.ca Circulation Inquiries info@hospitalnews.com
Director of Print Media

Lauren Reid-Sachs
ADVISORY BOARD
Barb Mildon, RN, PHD, CHE VP Professional Practice & Research & CNE, Ontario Shores Centre for Mental Health Sciences
Helen Reilly, Publicist Health-Care Communications
Bobbi Greenberg, Health care communications
Sarah Quadri Magnotta, Health care communications
Dr. Cory Ross, B.A., MS.C., DC, CSM (OXON), MBA, CHE Vice President, Academic George Brown College, Toronto, ON
ASSOCIATE PARTNERS:
Hospital News is published for hospital health-care professionals, patients, visitors and students. It is available free of charge from distribution racks in hospitals in Ontario. Bulk subscriptions are available for hospitals outside Ontario.
The statements, opinions and viewpoints made or expressed by the writers do not necessarily represent the opinions and views of Hospital News, or the publishers.
Hospital News and Members of the Advisory Board assume no responsibility or liability for claims, statements, opinions or views, written or reported by its contributing writers, including product or service information that is advertised.
Changes of address, notices, subscriptions orders and undeliverable address notifications. Subscription rate in Canada for single copies is $29.40 per year. Send enquiries to: subscriptions@ hospitalnews.com
Canadian Publications mail sales product agreement number 42578518.

4 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com
First-in-Canada procedure seeks to remove thyroid nodules with reduced side effects
For patients with thyroid tumours, surgery can be intimidating, invasive and, in some cases, even life-altering.
An innovative procedure called radiofrequency ablation (RFA) could offer patients a less invasive option that doesn’t require surgery and reduces the potential for undesirable side effects.
This procedure was performed for the first time in Canada by Dr. Jesse Pasternak, a surgeon at the Endocrine Clinic at Princess Margaret Cancer Centre and UHN’s Sprott Department of Surgery.
RFA is commonly used for chronic lower back pain, neck and arthritic joints, and its use on thyroids is currently approved to remove large or cancerous thyroid nodules. Dr. Pasternak is conducting a clinical trial to support the use of this procedure on small, suspicious nodules.
“The goal of this research is to get this treatment approved to provide the least invasive options to the most patients,” he says.
The procedure will also help reduce the surgical backlog.
“As we transition patients from a surgical waitlist to an hour-long procedure with no in-hospital recovery time, those surgical spots can be filled with patients with other, more concerning types of cancer who can now get treatment,” says Dr. Pasternak.

A thyroidectomy, the surgery that often removes nodules, can lead to a number of undesirable side effects, such as loss of thyroid function and cosmetic concerns for patients with post-thyroidectomy scarring. Dr. Pasternak has been exploring minimally invasive removal options for decades and is motivated by a desire to offer patients options and allow his patients more flexibility in their treatment.
“For patients who are not candidates for or don’t want surgery, radiofrequency ablation is a potential solution to directly target the nodule with no negative effects to the thyroid,” he says.
The RFA procedure preserves thyroid function and leaves the patient without a scar.
A FIRST-IN-CANADA MILESTONE
The first RFA procedure for a thyroid nodule in Canada was completed April 20 of this year. Deborah Guitmann Mutchnik was 52 when a thyroid nodule she had been monitoring for seven years started to become worrisome. When she found out she was eligible for this study, she jumped at the opportunity.
“I was calling them every two weeks, trying to schedule an appointment,” she says. “I don’t like surgery, so this was a perfect alternative.”
“For patients who are not candidates for or don’t want surgery, radiofrequency ablation is a potential solution to directly target the nodule with no negative effects to the thyroid.”
Thyroid nodules are very common, occurring in more than 50 per cent of people during their lifetime. A thyroid nodule is a solid or fluid-filled lump that forms within the thyroid. While many do not cause symptoms, they can grow large enough to cause pain, difficulty swallowing, cosmetic concerns and even lead to thyroid cancer.
Patients are often left with the choice of dealing with these symptoms until they become a larger issue, or undergoing invasive neck surgery.
In a thyroid radiofrequency ablation procedure, an ultrasound is used to guide a small needle directly into the thyroid nodule. The tip of the needle is heated with radiofrequency energy which destroys the nodule and kickstarts a shrinking process.
RFA is intended to reduce the size of a nodule to a point where symptoms no longer affect the patients’ day-today life.
Deborah’s study treatment has shown a reduction in the size of her thyroid nodule in follow-up appoint-
ments, paving the way for more procedures to be completed in the following weeks.
The recovery time was so minimal for Deborah that she actually did it in the middle of her vacation.
“I flew from Florida to get the procedure done, and the next day, I flew back,” she says. “Dr. Pasternak made sure I was very comfortable every step of the way.”
The study is seeking to find whether the RFA procedure can entirely elimi-

nate smaller nodules. It also would allow patients to have suspicious nodules treated before they have the chance to grow into something more dangerous.
“I am very proud to have been a part of this study that has the potential to provide solutions to others in need,” Deborah says.
Dr. Pasternak and his team hope their pioneering research will allow this procedure to become widespread in Canada to provide more options to patients everywhere. n H
AUGUST 2023 HOSPITAL NEWS 5 www.hospitalnews.com COVER
THE FIRST RFA PROCEDURE FOR A THYROID NODULE IN CANADA WAS COMPLETED APRIL 20 OF THIS YEAR.
Survey finds Ontario is at risk of greater loss of care
The Registered Practical Nurses Association of Ontario (WeRPN) is sounding the alarm, with new findings from their annual survey, “The State of Nursing in Ontario: A 2023 Review.” Based on insights from over 1,200 RPNs’ experiences over the last year, the research indicates that patient care is worsening due to dire staffing shortages, as Ontario’s healthcare system finds itself on the verge of collapse.
The survey found that 92 per cent of nurses say their workload has increased over the last few years – a figure that is higher than it was at the height of the pandemic. While 91 per cent of nurses in the province have directly witnessed patient care being negatively impacted due to continuously deteriorating staffing issues. The most alarming revelation – that Ontario could experience a greater loss of nursing care, as the harsh realities of the healthcare crisis are driving many nurses away from patient care on the front lines, prompting some to consider leaving the province, and some to consider leaving the profession entirely.
While Ontario may be reporting a slight increase in net registration numbers, those numbers don’t tell the full story. According to a report from the provincial nursing regulator, nurses leaving the province have continuously increased – during the same period, close to 10,000 Ontario nurses
Continued from page 4
opted not to renew their registration. Knowing that net registrations are determined based on the net change by subtracting the total number of losses from gains too, this shows why it’s important to dig deeper.
Topline findings from WeRPN’s survey include:
• Patient care is being compromised
– Nearly 7 in 10 nurses surveyed (68%) do not feel they have the time and resources available to provide adequate care to their patients.
– Among these nurses, 83 per cent are seeing increased wait times for patients, and 70 per cent have noted that it has gotten harder for patients to receive access to the necessary care they need, such as surgeries and diagnostics.
– A disturbing 62 per cent of nurses say they’ve directly witnessed how delays in such assessments have resulted in a decline in patient health.
• There could be a mass exodus of nurses leaving the province
– Over 6 in 10 Ontario nurses (62%) say they will, or they are considering leaving nursing. Among those who intend to leave, 59 per cent plan to leave the profession altogether, and 86 per cent intend to leave within the next two years. Some nurses are also shifting their practice – 38 per cent have changed roles in healthcare in the last two years, and within that group, 40 per cent have transitioned away from a direct patient care role.
Difficult pill to swallow?
In answering the PDQ, patients are being asked how they want to be seen or understood as a person by their healthcare team. These conversations are summarized into a few paragraphs, and with the patient’s approval, placed on their medical chart.
While mostly used in patients with serious illness, the PDQ is relevant across all of medicine.
Whether you are being seen for routine medical care, or find yourself moving towards the end of life,
or somewhere in between, who you are and acknowledgement of who you are as a person, matters. And the things that people disclose by way of the PDQ profoundly change the way healthcare providers see them. I’m a survivor of childhood abuse. My son is battling cancer. I am afraid to die alone. I am a former department head of medicine.
During the COVID-19 pandemic, the daughter of a women on a ventilator in intensive care shared that her
• Ontario’s nursing profession is in jeopardy
– One in five nurses (19%) are considering moving outside of Ontario to practice nursing. This trend is in line with recent data that shows a yearover-year increase in Ontario nurses not renewing their license.
– More than half of all nurses surveyed (54%) are considering leaving their current role to work for a private agency
– Compensation is top of mind for both agency (95%) and out of province considerations (83%).
• Pride in nursing has dramatically eroded since the pandemic
– 91 per cent of nurses say their daily experiences in the workplace have become significantly more stressful, and almost all (97%) say working short staffed has negatively impacted their workplace culture.
– In 2020, 67 per cent of nurses in Ontario said they had never been more proud to be an RPN. Sadly, three years later, pride in nursing has plummeted to a mere 31 per cent. n H
Prescribing psychostimulants for people at risk of overdose
Growing evidence supports prescribing psychostimulant medications to help reduce use of illegal stimulants such as methamphetamine, authors write in a CMAJ (Canadian Medical Association Journal) commentary.
Illegal stimulant use is rising, judging by the presence of these drugs in at least half of all opioid deaths in Canada in 2022.
Following evidence from clinical trials in Australia, Europe and the United States, physicians and nurse practitioners in Canada and other countries are increasingly prescribing psychostimulants as harm reduction for stimulant use disorder.
“This emerging evidence can support prescribers’ level of confidence in off-label prescribing of psychostimulants to patients with stimulant use disorder (and particularly for patients with attention-deficit/hyperactivity disorder and stimulant use disorder),” write Drs. Heather Palis, University of British Columbia and Scott MacDonald, Providence Health Care, Vancouver, BC.
In 2020, Canada’s Federal Minister of Health issued a letter to the provinces and territories to encourage increasing access to safer pharmaceutical-grade drugs as an alternative to contaminated illegal drugs. Only BC has issued guidance on prescribing psychostimulants to people at risk of overdose.
mother had survived the likely murder of her first child and was a spiritual leader in her community. She said that responding to the PDQ gave her a way of letting the healthcare team know that her mother “was no ordinary person.”
These kind of disclosures profoundly and forever change the healthcare provider’s lens, bringing an appreciation of who patients are as persons, above and beyond whatever ailment brought them to medical attention.
This is good for healthcare providers, helping stave off emotional indifference that can lead to professional burnout, while restoring human connection with the potential for them to be more whole themselves.
It is also good for patients and families, ensuring that patienthood doesn’t overshadow personhood.
Being a patient is hard, especially when it undermines your feeling that you are still you. That, it turns out, is the hardest pill to swallow of all. n H
Dr. Harvey Max Chochinov is a distinguished professor of psychiatry at the University of Manitoba, and author of Dignity in Care: The Human Side of Medicine, recently published by Oxford University Press.
6 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com IN BRIEF
Children and adolescents in food-insecure homes had more mental health visits
Children and adolescents living in food-insecure households had a 55 per cent higher frequency of physician visits for mental health reasons than those with adequate food supplies, according to new research published in CMAJ (Canadian Medical Association Journal). In 2021, almost six million people in Canada, including 1.4 million children and adolescents younger than 18 years faced food insecurity; that is, inadequate food intake because of financial problems.
To help implement prescribed psychostimulants in Canada, the authors suggest that clinical practice guidance should be updated based on new evidence, and that substance use treatment programs and clinics establish protocols to incorporate psychostimulants into the range of interventions.
“Broader implementation of prescribed psychostimulants as an effective option in the continuum of care for stimulant use disorder is needed in Canada; this practice would help the growing number of patients seeking to reduce their reliance on the illegal stimulant supply during the ongoing unregulated drug poisoning crisis,” they conclude.

“Incorporating prescription psychostimulants into the continuum of care for people with stimulant use disorder in Canada” was published July 17, 2023. n H
The study looked at population health survey data from the Canadian Community Health Survey on 32,321 children and adolescents linked to Ontario health care data. Researchers used a validated measurement tool to categorize household food access as food-secure, marginally food-insecure, moderately food-insecure, or severely food-insecure.
Of the total, 5216 (16.1%) were living in food-insecure, 1952 (6.0%) in marginally food-insecure, 2348 (7.3%) in moderately food-insecure and 916 (2.8%) in severely food-insecure households.
Researchers also found that children and adolescents in food-insecure homes had a 74 per cent higher prevalence of past-year acute care visits, defined as an emergency department visit or hospitalization for a mental or substance use disorder. The most common visits were for neurodevelopmental disorders, mood and anxiety disorders followed by social problems and other mental health issues.
“The coexistence of household food insecurity and service use for mental and substance use disorders here is problematic, given that both of these conditions have each been found to have negative consequences for social, educational and developmental outcomes among children and adolescents,” writes Kelly Anderson, associate professor of epidemiology and biostatistics at Western University’s Schulich School of Medicine & Dentistry, Canada Research Chair in public mental health research, and adjunct scientist at ICES Western.
“Taken together, these findings are concerning, and we need strong public policy to support families who face food insecurity,” says senior author Salimah Shariff, staff scientist at ICES Western. “As well, public mental health strategies must be improved and targeted to youth specifically to help reduce the strain on the public mental health system.”
The authors note that the findings may not apply to First Nations groups and people in remote regions where food insecurity is particularly high, or to jurisdictions beyond Ontario. The data are also almost a decade old, and
food insecurity has increased in recent years, especially during the COVID-19 pandemic.
The relationship between food insecurity and mental health issues may be more complicated, as a related commentary suggests.
“Given the diverse mental health conditions examined, it is unlikely that the mechanism of harm is lack of specific nutrients or poor diet quality,” writes Dr. Lynn McIntyre, Professor Emerita of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta. “Much more likely is that food insecurity contributes to mental distress among those living in difficult circumstances, as has been shown in studies of the relationship between severity of household food insecurity and mental health disorders among adults.”
Reducing food insecurity may help alleviate some mental health issues for children and youth.
“Clinicians should advocate as vociferously about the need for income security for families who are food-insecure as they do for solutions to emergency departments being filled with patients who need primary health care. Some jurisdictions have proposed that practitioners screen patients for financial strain and take steps to ensure that those identified as such receive their financial entitlements,” concludes Dr. McIntyre.
“Household food insecurity and health service use for mental and substance use disorders among children and adolescent in Ontario, Canada” was published July 24, 2023. n H
Be a change agent
and
C HANGE through unity and action 3 Join now and get MONTHS FREE JOIN NOW at join.RNAO.ca or call us at 1-800-268-7199 Applications will be dated per date of receipt. Special offer applies to new or lapsed members applying for 2023-2024 membership year. with PLP included
through unity
action
AUGUST 2023 HOSPITAL NEWS 7 www.hospitalnews.com IN BRIEF
“CLINICIANS SHOULD ADVOCATE AS VOCIFEROUSLY ABOUT THE NEED FOR INCOME SECURITY FOR FAMILIES WHO ARE FOODINSECURE AS THEY DO FOR SOLUTIONS TO EMERGENCY DEPARTMENTS BEING FILLED WITH PATIENTS WHO NEED PRIMARY HEALTH CARE.
Balancing technological promises
with effective healthcare management
By Shash Anand
The healthcare industry’s commitment to protecting patient privacy and adhering to the principle of “first, do no harm” is well-known. But how is technology supporting this commitment? Recent research from a SOTI report titled “The Technology Lifeline: Charting Digital Progress in Healthcare,” highlights a concerning trend. More than half (64%) of Canadian healthcare providers have experienced one or more security breaches since 2021, challenging how technology is used in healthcare.
Healthcare organizations and providers have a legal and ethical duty to ensure the security of patient information. Nonetheless, statistics reveal that within the past year, 32 per cent of Canadian healthcare organizations have suffered deliberate or accidental data leaks caused by employees. It was also found that 37 per cent of Canadian healthcare organizations have fallen victim to data breaches from external sources or DDoS attacks.
THE NEED TO STREAMLINE OPERATIONS
In response to the need to streamline operations, enable remote or hybrid work environments and support telehealth, there has been an accelerated push to use advanced mobile technology and implement bring-your-owndevice (BYOD) policies in healthcare. The adoption of automation through Artificial Intelligence (AI) and Internet of Things (IoT) are further transforming the industry, prompting organizations to rethink their technological priorities and advancements.
The proliferation and diversification of device implementation in healthcare continues to expand. According to data, 37 per cent of IT professionals have reported an increase in the us-
age of devices such as devices, tablets, rugged equipment and printers within their organizations over the past year. Additionally, 28 per cent have witnessed a rise in the use of personal devices for accessing company systems and networks.
IT INTEGRATION AND LEGACY SYSTEM TRANSITION CHALLENGES
As these emerging technologies become more prevalent, concerns regarding their integration and management alongside legacy systems have become apparent. An overwhelming 93 per cent of Canadian healthcare IT professionals have acknowledged the presence of legacy technology and processes within their organizations. Consequently, the top concerns faced by IT professionals due to legacy technology includes security attacks (39%), excessive time spent on issue resolution (37%) and the inability to access patient data quickly (25%).
To ensure the smooth adoption of new technologies, it is crucial to introduce robust security processes and review Enterprise Mobile Management (EMM) strategies and solutions. This tool will enable IT teams to monitor device usage, gain intelligence about the operations and promptly address issues as they arise in near real-time. Failure to do so may result in administrative lapses, maintenance struggles, device downtime, compromised efficiency and suboptimal patient care.
NAVIGATING THE HEALTHCARE IT PARADOX
Frontline healthcare workers have demonstrated immense dedication to patient safety, while healthcare IT workers have faced the formidable task of implementing new technologies within outdated backend systems and platforms. However, despite reports
indicating that 82 per cent of healthcare IT professionals have utilized tablets or laptops and 81 per cent have used smartphones in the past year, the effective management of these devices remains crucial.
Fifty-one percent of healthcare IT workers struggle to detect new devices, provide remote support or gather detailed information on device usage due to limitations imposed by legacy IT infrastructure. The report also found that 54 per cent of healthcare IT professionals find themselves consumed by resolving issues, leaving insufficient time for critical IT tasks. This imbalance highlights the paradox faced by the healthcare industry, where the rapid adoption of diverse devices for improved patient care outcomes coexists with inadequate resources to effectively manage and secure these devices.
PRIORITIZING INNOVATION AMIDST SECURITY CONCERNS
While security concerns persist within the healthcare sector, an overwhelming majority of IT professionals (83%) view the use of new technologies to enhance organizational efficiency and patient care outcomes as a top priority. Furthermore, AI and VR are actively being explored, with 67 per cent of IT professionals indicating that their healthcare organizations are in the research or implementation phases of these transformative solutions.
THE SHIFT TOWARDS AUTOMATION
The industry is witnessing a growing shift towards automating manual processes. Nearly half of the surveyed professionals have identified various manual tasks within their organizations that could benefit from automation. This includes data collection during patient visits (49%), accessing medical information/resources (43%),
updating patient records (45%) and retrieving test results (41%).
HARNESSING TECHNOLOGY’S FULL POTENTIAL
Research conducted by SOTI highlights that on average, each employee loses 3.4 hours per week due to technical or system difficulties, impeding technology’s potential to enable smoother, more secure and faster care delivery. To harness the full potential of technologies (such as laptops, smartphones, printers, scanners, RFID readers, AI and VR), effective integration, device management, upgrades and maintenance are imperative. Moreover, real-time data insights and remote monitoring of individual device performance also play a critical role to support new technologies.
EMBRACING LIFE SAVING TOOLS AND TECHNOLOGIES
The healthcare industry possesses an unprecedented array of lifesaving tools and technologies. To fully leverage their impact, organizations must “increase the dose” of technology utilized for patient care while fortifying the tools required to secure the collected data. Implementation of advanced diagnostic intelligence solutions provides performance visibility, predictability and remote device support, empowering healthcare professionals to deliver care more efficiently, reduce frustration and minimize errors.
Striking the delicate balance between innovation and effective management is essential in shaping the industry’s future. By embracing transformative technologies, optimizing device management strategies and enhancing connectivity, organizations can unlock the potential of technology, revolutionizing patient care and creating a secure, efficient healthcare ecosystem.n H
SPONSORED CONTENT 8 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com
Shash Anand, SVP of Product Strategy, SOTI. As SVP of Product Strategy at SOTI. Shash Anand oversees the company’s evolution from a single product centered around Mobile Device Management (MDM) to an integrated platform that solves many of the challenges around Enterprise Mobility Management (EMM).
An all-round win for students and employers alike
The mutual benefits of University of Toronto Scarborough’s Co-op job program
By Diana Swift
magine having a pipeline to a broad employee pool of young, flexible energetic people. Of enquiring minds studying many academic disciplines and eager to supplement university learning with real-world experiences in the healthcare setting.
These are resources healthcare administrators and researchers can tap into with student job recruitment through the University of Toronto Scarborough (UTSC) Arts and Science Co-op work program.

The Co-op program goes beyond a traditional internship, in which students may work as paid or unpaid aides over the summer break. A Co-op employment program supports students in their second and above year of study in their chosen field in connecting with temporary employment opportunities to the mutual benefit of both. “Our program has been facilitating this process between employers and students coming up on 50 years,” said Siobhan Flanagan-Dell, an External Relations Officer in the Co-op Program. “We have students from more than 35 academic program streams.”
These streams include, among others, life and social sciences, psychology, mental health and health policy, as well as computer science, mathematics, linguistics, philosophy, and literature.
THE CO-OP MODEL
Facilitated by UTSC’s Co-op program, students after their first year complete two to three employment experiences throughout their degree. They can take flexible terms of 4, 8, 12, or 16 months starting in January, May, or September. They take paid positions in business, industry, social services, and healthcare before returning to their studies.
The recruiting process has sent students into many healthcare facilities, including Sunnybrook Health Sciences Centre, The Hospital for Sick Children, University Health Network (UHN), Centre for Addiction and Mental Health (CAMH), and Unity Health Toronto, as well as private-sec-
tor companies such as Sanofi Canada and STEMCELL Technologies.
In the healthcare setting, Co-op-facilitated hires have done everything from lab work to research study support, recruiting patients and administering tests, as well as scheduling, analyzing data, and assisting with reports and presentations. They’ve handled analytics and worked in software development. To all of these assignments, they’ve brought competence, rapid learning, flexibility, and up-todate familiarity with current trends and methodologies.
FILLING THE GAP
Testimony to this is the experience of Jed A. Meltzer, PhD, a neurorehabilitation scientist at the Rotman Research Institute – Baycrest Centre in Toronto. “I recruit in life sciences and psychology. The students I’ve hired have been highly motivated, organized, and skilled in the demanding technical challenges in our lab,” he said. “Many of them have done fairly sophisticated computer programming tasks for us, and some have learned to do this on the job despite not having much prior experience.”
Dr. Meltzer described how a UTSC Co-op student stepped into the breach when a full-time research assistant left to carry on a complex 18-month project on language learning in seniors. “The student mastered all the complex tasks required to keep the study going and excelled at training a third person to finish up some remaining tasks after she had finished. Co-op students are a great choice for general support in a research lab, especially for filling in gaps between hiring more long-term personnel,” he said.
REAL-WORLD LEARNING
It’s a classic win-win scenario: the students get much-needed practical experience and income and, as an added benefit, an opportunity to refine their career goals.
For some, a co-op work term reinforces their commitment to their chosen field. “For others, the real-world
exposure may open up new interests and trigger a change in career direction,” Ms. Flanagan-Dell said.
A case in point is Joshua Jacob, a molecular biology and technology coop student placed at Sanofi Canada, where he learned a great deal about the pharmaceutical industry, particularly the vaccine development process. “My exposure to the industry left me excited to go back to school to relate what I learned at Sanofi to my studies,” Mr. Jacob said. “It has given me a wider perspective on my own career journey. I now appreciate being under pressure and pushed by my colleagues to be accurate and detail-orientated in completing deliverables.” He is now considering postgraduate studies with a focus on vaccine process/method and biotechnology.
Either way, employers get high-quality support and a link to a pool of potential full-time staff already knowledgable about their particular workplace operations and culture. In an era when retaining trained staff can be an issue for employers, some students will continue to work part-time after returning to school and some bring their experience back to you in a full-time position after graduation.
The recruitment process also serves students as a dress rehearsal for the fine art of successfully seeking permanent positions after graduation, Ms. Flanagan-Dell said. “We maintain a job posting board and streamline the application process, but students must do the work of applying and putting their best foot forward themselves.”
No matter their academic specialty, these students have transferrable skills that can support staff capacity in the hospital setting,” she said. “They’re eager to take on as much as they can and they bring enthusiasm and fresh perspectives to it. ”
FINANCIAL SUPPORT
Employers who hire UTSC Co-op program students may be eligible for tax credits or hiring grants/subsidies. UTSC can advise employers on these opportunities and connect them with funding organizations. For funding information visit: https://www.utsc.utoronto.ca/hire-coop/funding-resources-co-op-employers
Further details on hiring a UTSC Co-op program student can be found at: https://www.utsc.utoronto.ca/hirecoop/how-hire-our-students n H
SPONSORED CONTENT I AUGUST 2023 HOSPITAL NEWS 9 www.hospitalnews.com
ALS diagnosis transforms
storyteller into advocate
By Lise Diebel
St. Catharines resident Steven Gallagher spent much of his career as a journalist before switching to public relations with the Niagara Health hospital network.
Then, in 2019, Gallagher found himself on the other side of the healthcare system as a patient diagnosed with an incurable illness that has drastically shortened his life expectancy.
“I often say that we all get curveballs thrown our way in life, but being diagnosed with ALS felt like a 100-mileper-hour fastball to the head,” says Gallagher, 50, who is no longer able to work due to the progressive nature of ALS. Instead, he’s focusing on raising awareness – including sharing his patient experience at Hamilton Health Sciences (HHS) ALS Clinic.

WHAT IS ALS?
Amyotrophic lateral sclerosis (ALS) is a disease that affects nerve cells in the

brain and spinal cord, causing loss of muscle control. It often starts with muscle twitching and weakness in a limb, or slurred speech. Eventually, it progresses to muscles needed to move, speak, eat and breathe. It gradually paralyzes people because their brain is no longer able to communicate with the muscles in their body. There is no known cure.
SUBTLE SIGNS
Gallagher started experiencing symptoms in November 2018. “I had been bowling with my then four-year-old daughter Olivia and noticed my hand was stiff and it was harder to move my thumb. A month or so later, I saw my family doctor who sent me for X-rays.”
Images showed signs of osteoarthritis, often called overuse arthritis because it’s caused by wear-and-tear. “That seemed logical to me, given my many years typing on a keyboard as a journalist and communications specialist,” says Gallagher.
Over the next few months, his hand stiffness grew worse. “One day, I was
having lunch with two orthopedic surgeons at the St. Catharines hospital where I worked. I asked them about my hand, wondering if it was something they could fix. They took the time to look at my hand and forearm and noticed slight muscle atrophy. They encouraged me to see a neurologist as soon as possible. I’m very grateful to them both for pointing me in the right direction.”
The Niagara Health neurologist referred Gallagher to the HHS ALS Clinic where the diagnosis was confirmed in August 2019.
“The diagnosis devastated me and my family at the beginning, but that darkness eventually turned to light because of many factors including the care provided by the ALS Clinic team at Hamilton Health Sciences.”
A LEADING CANADIAN CLINIC
The HHS ALS Clinic is among the largest in Canada, and one of only five in the province. It was founded by
neurologist Dr. John Turnbull in the early 1990s. Today, Turnbull is one of three clinic neurologists along with Dr. Marvin Chum and Dr. Matthew Gladman. The core team also includes nurse coordinator Barb Miller, social worker Suzanne Zietsma and respiratory therapist Jenneca Herceg. They also connect patients to hospital and community support needed to live safely and independently at home. Gastroenterologist Dr. Siwar Albashir, physical medicine and rehabilitation specialist Dr. Adrian Opala and respirologist Dr. Andreas Freitag also play key roles in supporting patients.
The clinic follows 250 to 300 patients at any one time from as far away as Kenora, Dryden, Sioux Lookout and Thunder Bay, with three to four new patients a week. It’s also one of the largest clinics in the country for research trials through a partnership with McMaster University.
Patients typically have clinic appointments every three months and
Photo: courtesy of the ALS Society of Canada
10 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com NEWS
can contact the team at any time as needed. The pandemic introduced secure telephone and video conferencing instead of in-person appointments, which is much easier for patients and their families.

“The team does an excellent job of keeping our patients out of hospital emergency departments and intensive care units by thinking ahead to their future needs, to help avoid a crisis,” says Turnbull. “This benefits the health-care system, the hospital and our patients who would much rather be at home than in a hospital bed.”
Team members form close relationships with patients and their families,” adds Miller. “ALS is a family disease because families provide so much support.”
Gallagher meets with the team every three months through video conferencing. “They guide me on my journey, always thinking a few steps ahead so my family and I are prepared for each stage of the disease,” he says. “They also make sure I’m receiving the latest medication to slow the progression.”
IMPROVED QUALITY OF LIFE THROUGH EARLY INTERVENTION
Early diagnosis is key to helping ALS patients enjoy the best quality of life for as long as possible, says Dr. Marvin Chum, Gallagher’s neurologist at the ALS Clinic.

Yet it’s common for people experiencing symptoms to circulate through the health-care system, undergoing numerous tests and specialist referrals before finally arriving at an ALS Clinic. Currently, in Canada, it can take two years or more for someone to be diagnosed with ALS, according to the ALS Society of Canada.
These patients don’t have the luxury of time, says Chum. “Half will pass away in three to four years from the time of symptom onset so it’s critically important that they’re diagnosed as early as possible and start taking medication to slow the disease’s progression.”
Chum encourages community physicians and specialists to immediately refer patients to the clinic if they suspect ALS. “There’s no need to order
tests or wait for results before referring to us. We can do all that here, very quickly.”
ADVOCATING FOR AWARENESS
After being diagnosed at the clinic, Gallagher immediately started taking medication to slow the disease. For the first year-and-a-half, his ALS progressed slowly. “It was really only my right hand that was impacted. I was still quite active – running, cycling
and playing golf and tennis.” In the spring of 2021, he started to experience breathing issues and by summer he used a cane to walk.
“Today, my overall mobility is very weak,” says Gallagher, adding that breathing has also become much more challenging and his speech is now impacted.
“Even as this disease slowly robs me of my speech, it will never silence me when it comes to advocating for advances in care.” n H
Lise Diebel works in communications at Hamilton Health Sciences.
The ALS Clinic team.
AUGUST 2023 HOSPITAL NEWS 11 www.hospitalnews.com NEWS
Photo: Josh Carey
Niagara Health research provides key insights for frontline healthcare workers about patient safety

When Virginia Pullar first noticed there seemed to be an unusually high number of patients falling in the hospital during the early part of the COVID-19 pandemic, she immediately wanted to investigate it further.
Her initiative led to a research project that provides key insights about patient safety for frontline workers. Findings from the project, “Exploring Changes in Patient Safety Incidents
During the COVID-19 Pandemic,” have been published in the Journal of Patient Safety. That research also garnered Pullar recognition for her enterprising use of data. The Co-ordinator in Decision Support received the Dr. Johan Viljoen Staff Research Award in May during Niagara Health’s annual Research Day.
During the pandemic, Pullar worked with the Niagara Health Falls Committee collecting data from the Incident Reporting System (IRS). IRS is a process for frontline staff to report incidents within the hospital, including patient falls.
The committee expected to see a drastic drop in the number of falls, given the decrease in people entering the hospital during the pandemic’s first wave.
“Most people were staying home,” Pullar says. “But when I actually looked at the data, it showed that we had more falls. We didn’t expect that.”
That led Pullar to investigate the data further. Thanks to Niagara Health being open to new ideas and innovative action, she quickly collaborated with members of the Anesthesiology Department and the Emergency Medicine Researchers of Niagara (EMRoN) team.
Having worked with this group of researchers in the past, Pullar says she wanted to take advantage of their experience in analysis and research writing. She knew they could apply the statistical model to fully understand if there was a significant change in the data. In addition, the team analysed all of the data, not just falls, to see if there was anything else they could learn.
“Leveraging the research team’s statistical expertise, and my knowledge of the data set, it was just a really good
fit, and it came together quite easily,” she says.
Once the data analysis was completed, Pullar says it was just one piece of the puzzle.
“It doesn’t give you the answers as to what is actually happening,” she says. “You still need the qualitative piece. So, we talked to different staff and different teams across Niagara Health.”
After all the information was gathered, Pullar took it back to the Falls Committee where it was theorized that visitor restrictions, and reduced patient contact and supervision may have had an impact on the number of patients falling.
“We weren’t going in and out of the rooms as frequently as we were before the pandemic because every time, you had to put on and take off your PPE,” she says. “So, maybe just the frequency
of how we were interacting with our patients had an impact.”
Overall, Pullar says the most important conclusion the data highlighted was the need for a rapid response and adaptability to unpredictable situations, particularly those that could arise during a pandemic.
“Even if we experience something on a smaller scale, we will now know to think about causes for more falls as being a potential impact for some of our patients,” she says.
Pullar credits diligent frontline staff for reporting the falls in the first place.
“It speaks to the culture of our organization, and the culture around safety, that staff are comfortable in reporting when things don’t go exactly as planned with a patient. Then we can learn from it. That’s how we change policy and process.”
Pullar says she simply wanted to show IRS data is valuable
for more than just day-to-day reporting.
“We use the data a lot, but this was the first time we had ever imported it into an analytical model. It has the potential for us to get valuable information back to the frontline staff working directly with the patients.”
What’s next? Pullar says the new hospital information system (HIS) and advancements in data collection will lead to improved patient experience. The HIS will also improve digital access for physicians and staff, and increase communication between team members with real-time documentation sharing.
“The more we can provide high-quality data in real time, the faster and more informed the decision makers, leadership, and frontline staff can be in making decisions for quality care and patient experience,” she says. n H
12 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com NEWS
Waterloo researchers developing first drug of its kind to treat incurable eye diseases
Researchers have developed a novel synthetic protein to treat macular degeneration and other incurable eye diseases that lead to blindness in millions of people. It is the first drug of its kind and is currently in human trials.

Neovascular age-related macular degeneration (AMD) affects more than 200 million people worldwide. In addition, millions more with type-1 or type-2 diabetes are at risk of developing diabetic macular edema (DME). Both diseases currently have no cure.
The novel antibody activates the Wnt-signaling network, a group of proteins that pass information into a cell through surface receptors such as frizzled receptors (FZD). It improves the blood vessel integrity in the eye and thereby blocks fluid buildup in the retina and may help improve sight in those afflicted with AMD or DME.
The drug originated in the lab of Dr. Sachdev Sidhu, entrepreneur in
residence researcher at the University of Waterloo’s School of Pharmacy. He led its development with AntlerA Therapeutics Inc., where he is a scientific co-founder, in partnership with EyeBio.
“While the biology of the Wnt/ FZD pathway in eye disease has been studied for many years, we are the first group to develop a drug that activates this pathway in patients, leading to a treatment for these diseases,” Sidhu said. “Our synthetically derived proteins can act like the natural proteins and we knew if we figured this out, we could open many other doors to treat other diseases.”
The researchers are now developing drugs that target other branches of the Wnt/FZD system and could treat other common diseases that affect people across the world, including diseases of the lungs, liver, bones and intestines.
“Basic science and drug development are closely linked due to the
advancement of technology and its ability to translate ideas rapidly into therapies for patients,” Sidhu said. “It is essential to have entrepreneurs involved in both innovative science and business for ideas to advance smoothly into products.”
The research team that developed the drug alongside Sidhu includes Dr. Jarrett Adams and Dr. Levi Blaz-
er, engineering and science research associates at Waterloo.
The team is confident this treatment will change the drug development landscape, as it is the first member of an entirely new class of drugs that can actually repair organ damage caused by degenerative diseases, rather than merely preventing further damage, as is the case with most current drugs. n H
New conference aims to address nationwide healthcare inequity
Uof T Scarborough and Scarborough Health Network (SHN) are hosting a new and innovative two-day conference, which will bring together presenters with clinical and research expertise, scholars and community perspectives.
Hosted at U of T Scarborough on October 13 and 14, the Building Communities through Inclusive Health conference aims to address the root causes and consequences of health inequities, the role of communities in promoting health equity, and policies and programs to support community solutions.

Addressing accessibility of care is critical to make it a truly accessible conference. As such, it will be free to all attendees (apart from those seeking Continuing Professional Development credits).
Throughout this two-day event, we will hear from ‘tri-perspectives’ of clinicians, scholars, and community members who will collaborate to bring meaningful discussions on how to bridge health inequities experienced by marginalized populations nationwide.
“Let’s challenge and change health inequities through research, innovation, and partnership,” says David Graham, President and CEO of SHN.
“This unique tri-perspective approach will provide a richer understanding of the interaction of social conditions and health, as well as their implications for achieving a more resilient and equitable health system.”
Speakers include Fiona Miller, Professor of Health Policy at the Dalla Lana School of Public Health; Sheila Blackstock, Associate Professor of Nursing at the University of North
British Columbia, and Adriana Carvalhal, Psychiatrist and Scientific Director, Scarborough Health Network Research Institute.
“Together, we will learn about the bold ideas, lessons and innovations that come from understanding the
healthcare needs of the underrepresented and underserved,” says Wisdom Tettey, Vice-President, University of Toronto and Principal, University of Toronto Scarborough.
To register for conference, please visit inclusivehealthconference.ca.n H
SPONSORED CONTENT AUGUST 2023 HOSPITAL NEWS 13 www.hospitalnews.com NEWS
Bearing witness: The power of presence
By Aline Demerjian

It was a routine day in our bustling critical care unit: alarms and phones ringing, staff rushing around doing the numerous things that need to be done at any given time. When suddenly, everything stopped. An eighteen-year-old had been brought in by ambulance, unresponsive. The young woman was stabilized enough to make the elevator trip one floor up to our unit. While the team continued their life saving interventions, I escorted her family upstairs. Our team’s efforts were unsuccessful; the young woman died in the presence of her mother, father, and younger brother. Time seemed to stand still. Everyone was distraught, but none more than that family.
I asked myself: what could we do in their moment of overwhelming grief? I distinctly remember going into the patient’s room where her mother was sitting in a chair near the bed, quietly crying. With tears in my own eyes, I crouched down in front of her, looked at her person to person. I could not imagine the pain she was experiencing. But I could silently communicate: “You are not alone. I see you. I see your pain.”
Times of crisis and immense emotional pain are hard to describe. The world stops and speeds up at the same time. It is unbearable yet inescapable. If you are lucky, you are not alone during these experiences. I am a social worker in a large critical care unit. Sadness and tragedy are our norm. We help families to make unbelievably difficult decisions and support them through the process. I cannot take their pain away, I cannot change their reality. However, I can stand with them, share with them, cry with them. I can bear witness.
Everyone wants to “do” something to help. But there is not always
something to “do.” Social workers are tasked with most things to do with emotions. Sometimes all I can do is be present. It feels helpless. But there are some ways to approach emotional suffering that can help: take their lead, give them space to be alone, make small talk, offer to call someone close. Focus on the here-and-now: offer water, a place to sit, physical proximity, a warm blanket. Get their questions answered by the medical team. Begin to prepare the family for the possibility of a bad outcome.
Social work is one of many helping professions in the hospital. Part of what makes our role unique is our focus on communication and relationship building. It takes time and trust to establish a connection with a person, one which would allow for the truth and hard work that must be shared. In a hospital setting, particularly in a busy critical care unit or emergency department, the social worker must be able establish rapport quickly. Empathy, openness, and calm must be conveyed within minutes to enable the building of trust. We are seeing people at their most vulnerable, when they are overwhelmed with both information and emotions, when they feel helpless. Our aim is to relieve that suffering, if only a little.
Grief presents in many ways, and we often don’t know what to do with it. There is loud noise coming from the family room and staff turn to me to fix it. We stop and listen for a moment: the noise is chanting, praying, crying. Teams tend to get very uncomfortable with outward expressions of emotion. But what is crying in this context if not an outward expression of the grief that someone is feeling? What is prayer if not an expression of hope? What is wailing, chanting, pacing, hand-wringing if not a way to let out the pain felt inside? We must make space for all these forms of expression for they are normal responses to tremendous anguish.
Patients in the critical care unit are usually too sick to be conscious. So I work with their families to discover the person we’ve been tasked to care for. My offer of “help” looks different for each family I support. I learn the patient and family’s value system, strengths, and barriers; because this informs how I engage and help them. I hear their story; I ask for their version of what is happening to their loved one. This often helps me understand how much they are absorbing of the reality unfolding in front of them.
A nurse is concerned two siblings aren’t grasping the gravity of their father’s stroke. I introduce myself, explain my role is to help support families when they have a loved one in the critical care unit. They tell me they want to know if their dad is going to need a cane or a walker when he comes home. I learn their dad is mom’s caregiver since her heart attack, so they don’t want her to see him till he is on the mend. He won’t mend – they’ve been told this, but they haven’t heard it yet. I hear them out, knowing their lives are being altered forever. It’s common that family members do not register what doctors
tell them. My work is to figure out why.
It is easier to deny tragedy than it is to feel its weight. But slowly, we move a little, together. Whether it is over minutes, hours, days, or longer, we will move to acceptance of this unbearable reality. Making space and giving time to get there is not easy. Sitting with those feelings and listening to the pleading, is not easy. And in time, we move, even just a little. “What if the doctor is right?” Then I will stand here with you, and we will hear the news together and we will figure out the next steps.
A man, in his seventies, a pillar of his community, steps out of the shower one morning, complaining of a weird feeling in half of his body. He suddenly collapses, an ambulance is called, and he is rushed to the hospital. Scans confirm he has experienced a sudden brain bleed. We watch him for days. His wife tells me she believes in miracles, she will not lose hope. “No,” I say, “we must always have hope for something.” I walk the journey with her from hope for recovery to anticipatory grief. I get to know the family. I sit with them as various doctors give them updates, always accompanied by a terrible prognosis. Some days, they cannot hear it. They don’t want to talk to the doctor again. “Tell me some good news” she says to me. But over days, she moves to acceptance. She cannot be the one to say the words, but through her son, she tells us, “I understand,” and we make a plan to remove her husband of over forty years from life support. “We are not far” I tell her as I leave the room. “You are not alone,” I convey.
It is imperative to know that we are not alone. The family must feel we care – about them and about what is happening. What we “do” is we care. Caring is doing. And sometimes, the only caring we can give, is bearing witness. n H
Aline Demerjian is a Social Worker at Lakeridge Health. This is an original manuscript of an article published by Taylor & Francis in the Journal of Social Work in End-of-Life & Palliative Care on June 2, 2023.
14 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com NEWS
A First hospital in the world to purchase Indigenous supplied, branded medical gloves
unique partnership initiated by Niagara Health has led to a global first while putting the hospital on the path toward economic reconciliation with Indigenous Peoples.
Niagara Health recently became the first hospital in the world to receive a shipment of Indigenous-supplied, acute care nitrile medical gloves. The gloves, manufactured by PRIMED Medical Products, are distributed exclusively by Certified Aboriginal Business Medical, Surgical and Safety Supplies (MSS) Ltd. through Mohawk Medbuy Corporation, a not-for-profit, shared services organization that pro
The gloves are also symbolic of Niagara Health’s commitment to economic reconciliation and implementing certain calls to action by the Truth and Reconciliation Commission.
The collaboration came to be after former Niagara Health board member and Mi’kmaw lawyer Bernd Christmas introduced Angela Zangari, Niagara Health Chief Financial Officer and Executive Vice-President, Finance, Redevelopment and Facilities, to MSS President James Hiebert. Both Christmas and Zangari were intent on following the federal government’s lead of achieving five per cent procurement from Indigenous businesses.
“I always had that idea that we should buy Indigenous products as best we can,” Zangari says. “Our goal was ‘How can we make this work?’ Even if it’s small steps, let’s make this
Zangari, who sits on the Mohawk Medbuy board, connected Hiebert with Tony DiEmanuele, the company’s President and CEO, to initiate
building an Indigenous value-based supply chain starting with MSS.
From there, Mohawk Medbuy introduced Hiebert and MSS to some of their contracted vendors, including PRIMED to see where the collaboration could go. The result was co-branded gloves that Mohawk Medbuy is now marketing to its member hospitals, explains Veronica Guido, Mohawk Medbuy’s Director of Indigenous Partnerships and Strategies.
“Without Niagara Health, that initial introduction to James wouldn’t have happened and it’s been a butterfly effect,” Guido says. “Now the gloves are here and it’s really exciting to see this come full circle and be a product that we’re seeing in hospital rooms. It’s a visible reminder that Indigenous Peoples are here, and Economic Reconciliation is possible and can happen if we put our minds to it and work to support Indigenous businesses and entrepreneurs.”
The social benefits of the partnership help more than one Indige-

nous-owned business succeed. As a social enterprise, MSS is committed to sharing half its net proceeds to further Economic Reconciliation of Indigenous communities by providing scholarships for youth in science, health and pre-medical programs in Canadian universities, including in Niagara.
MSS will also work with Indigenous communities, leaders and elders to develop business opportunities, and work with Indigenous healthcare centres to ensure safe, accessible care that includes traditional healing and a trauma-informed approach to care.
“We talk about the past and present and what the future can look like,” Hiebert says. “This shows what we can do for communities and economies. And really, it’s all about delivering healthcare and adding the value of being involved in the community. We want to be at the table so we can increase the influence of Indigenous Peoples in healthcare in Canada and across the globe.”
n
H
AUGUST 2023 HOSPITAL NEWS 15 www.hospitalnews.com NEWS
Transforming Canada’s healthcare system must begin with children
By Emily Gruenwoldt
Never events” have become normalized in Canada’s children’s hospitals (and beyond) as children and youth struggle to access essential and time-sensitive healthcare services.
Every child deserves the opportunity to grow up healthy and strong, and to reach their full potential. But systemic underinvestment in the health and well-being of our youngest citizens has left them vulnerable.
Today, Canada dedicates 1.68 per cent of gross domestic product (GDP) to policies and investments focused on children and youth, while other nations (like France, the United Kingdom and Sweden) invest up to 3.68 per cent. This has contributed to Canada’s unenviable ranking of 30th amongst 38 wealthy countries with respect to the overall health and well-being of children and youth. Status quo is not an option.

Following a historic viral season last fall, and in the wake of untenable backlogs for surgical and diagnostic services, the federal government pledged an immediate $2-billion Canada Health Transfer top-up to address “immediate pressures on the health care system, especially in pediatric hospitals and emergency rooms, and long wait times for surgeries.” This is an important acknowledgment that investments are needed to ‘right-size’ children’s health systems.
Unfortunately, to date, only two jurisdictions (Ontario and Nova Scotia) have taken steps to commit earmarked funding to strengthen the capacity of children’s healthcare systems. It’s critical that all provinces and territories share a commitment to achieving meaningful improvements in children’s health service delivery.
On July 19, 2023 the Ontario government did just this – announcing unprecedented funding earmarked for children’s health systems – including children’s hospitals, but also community- based child development and mental health service provider organi-


zations. These dollars will have immediate impact addressing long backlogs for urgent and essential services, but also creating capacity for tomorrow.
Measurably improving children’s health outcomes, however, is not a task for the provinces and territories alone. It requires a collective and collaborative effort between our federal, provincial, territorial, and Indigenous governments to move towards a shared vision of healthier futures for our children. From there, we must direct predictable and ongoing funding towards children’s healthcare providers, creating much-needed relief for the struggling children’s healthcare system.
We must immediately start looking beyond the crisis to where Canada needs to go next. That means shifting from defining the problem to imple-
menting solutions, including the development of a pan-Canadian child health strategy, and establishing predictable and ongoing funding to begin ‘right-sizing’ children’s health. Above all, we need action-oriented leadership to effect meaningful, long-term change.
A transformative child health strategy addressing not only physical health but also mental health and other essential services is the key to elevating the well-being of Canada’s children and youth. By setting clear targets, regularly measuring outcomes, and committing significant funding over the next decade, such a strategy can make substantial progress in improving the health and well-being of our children.
Leadership also plays a crucial role in driving this change. We need leaders who are passionate about improv-
ing health outcomes for children, and who are willing to work collaboratively across all levels of government and with community partners. Their action-oriented focus should prioritize accountability, transparency, and continuous improvement in the delivery of children’s healthcare services.
Time is of the essence – everyday matters in the life of a child. The opportunity to make a sizeable and immediate impact on children’s health and wellbeing is within reach. Together as a child health community we have well defined the challenges, but equally have great line of sight into the solutions. We all have a role to play reimagining, and indeed transforming healthcare services for children, youth and their families, but we need our government partners at the table.
n
“
H
16 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com PAEDIATRICS
Emily Gruenwoldt is President & CEO, Children’s Healthcare Canada and Executive Director, Pediatric Chairs of Canada.
Caring for families close to home
By Marie Sanderson
Shylee giggles enthusiastically, surrounded by toys, as her mom packs a diaper bag. “There’s a lot to cart around when we go out – her oxygen tank is the most important,” says Shanice, who looks proudly at her daughter, who was born at 24 weeks at Sunnybrook.
The pair are on their way to see the care team at Sunnybrook’s Neonatal Follow-Up Clinic. Shylee still uses oxygen for pulmonary hypertension and continues to smile as they hop in the car. Thankfully, their commute is just a ten-minute drive to a satellite clinic which sees patients in the Peel region once a month.
“Convenience-wise, it’s absolutely incredible,” says Shanice, who lives in Brampton and is grateful to have access to a clinic so close, with the same care team she’s known since Shylee’s four month stay in Sunnybrook’s neonatal intensive care unit (NICU). “The clinic has all of the same staff we’ve came to know – it’s reassuring knowing we have access to this expertise close to home.”
Babies like Shylee, born at less than 30 weeks, and those who had complicated stays in the NICU, are seen in person and virtually by the follow-up clinic. Two satellite clinics, in Whitby and Brampton, provide accessible care for those who don’t live close to the main hospital when it comes time for an in-person visit.

“Sunnybrook’s NICU isn’t a postal code unit,” explains Dr. Rudaina Banihani, Medical Director of the Neonatal Follow-Up Clinic and a Neonatologist and Developmental Behavioural Pediatrician. “Our NICU is a level three unit, which means we care for the most premature and sickest babies from across the province. This model of care, where babies and families are seen close to home, really sets us apart.”
The model is longstanding, with the first satellite set up in the 1990s by Dr. Elizabeth Asztalos, a neonatologist with specialty in developmental pediatrics with the DAN Women & Babies Program. Satellite clinic visits comprise roughly 20 per cent of the clinic visits each month. The care team provide routine check-ins from the time a child is discharged from the hospital up until school age. Care in the clinic focuses on supporting each child’s developmental potential, by looking closely at motor skills, communication, engagement with the environment, and other important milestones. The clinic also prioritizes overall family well-being.
Dr. Banihani is quick to note the care doesn’t replace a child’s pediatrician, who are always the first line of call for acute care issues. That said, the team consults and collaborates with other health care professionals, such as pediatricians, to identify each child’s strengths and areas for growth.

The Dhaliwal family are big fans of the model of follow-up care. Ranvir was born at 29 weeks and is now a very active six-year-old and a “bright spirit who has so much energy”. At Ranvir’s age, visits focus on the transition to grade level schooling, learning skills and peer relationships to support academic success and enjoyment of learning, as well as friendship building.
“Relaxed, comfy and no stress – that’s what it’s like visiting the satellite clinic,” says Kiranpal, Ranvir’s mom. “I know we’re getting the developmental support we need, and it’s close to our house. For Ranvir, it’s a lot of fun as there are so many toys and he gets to play.”
The interdisciplinary team is comprised of physicians with a knowledge of neonatal and developmental care, occupational and physical therapists,




speech and language pathologists, and a registered nurse. All care providers specialize in the care of preterm infants and strive to collaborate with each family.
“From feeding, to sleeping to toileting, we are focused on each child’s development related to their prematurity,” adds Dr. Banihani. “It’s fulfilling
to meet families at different points in their child’s journey, from the hospital to starting school and beyond.”
For kids like Shylee and Ranvir, a visit to the clinic is all about play. “It looks like a play place – it’s bright and colorful. And we get to see familiar faces who truly support and cheer us on,” says Shylee. n H
 Marie Sanderson is a Communications Advisor at Sunnybrook Health Sciences Centre.
Shylee, a patient of the clinic, during her time in Sunnybrook’s NICU and present day.
Photo: Shanice Hutchinson
Team members of Sunnybrook’s Neonatal Follow-Up Clinic.
Marie Sanderson is a Communications Advisor at Sunnybrook Health Sciences Centre.
Shylee, a patient of the clinic, during her time in Sunnybrook’s NICU and present day.
Photo: Shanice Hutchinson
Team members of Sunnybrook’s Neonatal Follow-Up Clinic.
AUGUST 2023 HOSPITAL NEWS 17 www.hospitalnews.com PAEDIATRICS
Photo: Kevin Van Paassen, Sunnybrook
New study finds subgroups of kids with similar brain patterns do not share diagnostic labels
Anew study led by Holland Bloorview Kids Rehabilitation Hospital found that groups of neurodiverse kids and youth who share similar brain patterns do not always have the same diagnosis.
The study was published in the Journal of the American Medical Association (JAMA) Network Open.
“These study findings suggest that our broad diagnostic labels do not always align with unique patterns of brain differences,” says Marlee Vandewouw, the study’s first author and a doctoral candidate at Holland Bloorview’s Autism Research Centre. “Brain-based groupings, like the ones found in this paper, instead can help to understand and support the unique strengths and needs of neurodivergent children.”
HOW THE STUDY WAS CONDUCTED
Vandewouw, Dr. Azadeh Kushki, the study’s principal investigator, and their research team examined two independent data sets from Ontario and the New York City area – POND (Province of Ontario Neurodevelopmental Network) and HBN (Healthy Brain Network).
Each dataset examined contained 551 male and female children and youth (5 to 19 years) with various neurodevelopmental conditions including autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), obsessive-compulsive disorder (OCD) as well as neurotypical (typically developing) kids.
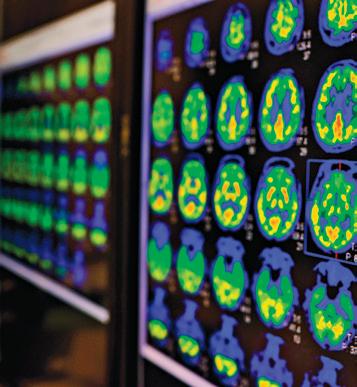
The research team used neuroimaging to examine the brain function in each child. Children with similar patterns of brain function were then grouped together using machine learn-
ing algorithms into smaller sub groups. The team then looked to see how groups of children who share similar brain function are similar in terms of their behavioral traits extracted from clinical and parent reports.
KEY FINDINGS
The research teams found that in both the POND and HBN data sets, the children and youth in who share brain patterns have different diagnoses. Thinking skills and traits like hyperactivity better described the subgroups than the diagnostic labels.
This is the first study to show that these similarities in brain patterns are found across two independent datasets, further showing the validity of the research team’s findings.
KEY TAKE AWAY
“The results of this study tell us that we need to consider the unique strengths and needs of each child, beyond broad diagnosis labels,” says
Dr. Kushki, who is a senior scientist at Holland Bloorview’s Bloorview Research Institute and associate professor at the University of Toronto.
“Ultimately, understanding brain differences and similarities can help us design more personalized approaches for supporting neurodivergent children.”
In the future, the research team hopes to conduct a similar study to understand how these subgroups may change as a child grows.
The research team also recognizes that having a diagnosis is very important in accessing services as well as being an important part of their identity.
“This study looked at how diagnostic labels are connected to biological constructs – how biologically similar a person’s brain may be to another person and if that’s reflected in our current labels– but it is also important to think about the reasons why our existing labels may be meaningful,”
says Dr. Kushki. “It is critical that the voices and preferences of neurodivergent communities are at the forefront of these conversations.”
“Current diagnostic labels are not necessarily helping us understand brain differences or biology of a child seeking help. Understanding which kids share brain and body biology is important in rethinking our diagnostic systems and how we organize our health care sectors to meet the needs and preferences of neurodivergent children and youth”, says Dr. Evdokia Anagnostou, the Principal Investigator for the POND Network, vice-president of research at Holland Bloorview and one of the study’s co-authors.
The study’s co-authors are: Jessica Brian, Holland Bloorview and University of Toronto; Jennifer Crosbie, University of Toronto and Hospital for Sick Children; Dr. Russell Schachar, University of Toronto and Hospital for Sick Children; Alana Iaboni, Holland Bloorview; Stelios Georgiades, McMaster University; Dr. Robert Nicolson, Western University; Elizabeth Kelley, Queen’s University; Dr. Muhammad Ayub, Queen’s University; Dr. Jessica Jones, Queen’s University; Margot Taylor, The Hospital for Sick Children, University of Toronto; Jason Lerch, The Hospital for Sick Children, University of Oxford, University of Toronto; Paul Arnold, University of Calgary; and Dr. Evdokia Anagnostou, Holland Bloorview, The Hospital for Sick Children, University of Toronto.
The study, Identifying Replicable Subgroups in Neurodevelopmental Conditions Using Resting-State Functional Magnetic Resonance Imaging Data, has been generously funded by POND, Canadian Institutes of Health Research and New Frontiers in Research Fund. n H
Holland Bloorview Kids Rehabilitation Hospital believes in creating a world where all youth and children belong. We are the only children’s rehabilitation hospital in Canada focused on combining world-class care, transformational research, and academic leadership in the field of child and youth rehabilitation and disability. We are a top 40 Canadian research hospital that is fully affiliated with the University of Toronto. Providing both inpatient and outpatient services, Holland Bloorview is renowned for its expertise in co-creating with clients and families to provide exceptional care and is the only organization to ever achieve 100 per cent in three successive quality surveys by Accreditation Canada. Holland Bloorview is a founding member of Kids Health Alliance, a network of partners working to create a high quality, consistent and coordinated approach to pediatric health care that is centred around children, youth and their families. Together we dream big. Together we champion a world of possibility. For more information or to donate, please visit hollandbloorview.ca or connect on Twitter, Facebook, Instagram, LinkedIn and the parent-blog BLOOM.

18 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com PAEDIATRICS
Supporting Canada’s sick children and their families by enabling family-centered care
The paediatric healthcare system across Canada has been facing significant strain, largely due to being underfunded and undersized. As Canada’s child population continues to grow, so too does the demand for child and youth health services. Add to this over two years of a global pandemic, resulting in cancelled procedures, staff shortages, and increased risk to children’s health and wellbeing – and it is evident why there’s a need to ‘rightsize’ the healthcare system to ensure all children receive the care they need.
For Ronald McDonald House Charities (RMHC) across Canada, the challenges faced throughout the healthcare landscape have prompted increased innovation, adaptation, and cooperation to ensure sick children and their families can access the medical care and supports they need. Over the last 40+ years, the RMHC mission to support families has grown and evolved from bed & breakfast style accommodation to family wellness centres found today. RMHC across Canada provides a place for families of sick children to sleep, eat, restore, and receive the support of community. With a well-cared for family by their side, sick children get stronger.
Today, RMHC is part of the fabric of Canada’s paediatric healthcare system and its network of 34 programs across the country serves more than 26,000 families from over 3,400 communities in an average year.
STRONGER TOGETHER
With over 450,000 families supported in the last 40+ years, RMHC across Canada is tightly woven into the communities we serve. From coast-tocoast-to-coast, in addition to having strong relationships with our hospital partners, we work closely with community partners, enabling the expansion of the breadth and depth of our national mission.
Across the country, RMHC mission delivery is a testament to the power of partnerships when it comes
to navigating this challenging environment together. There is strength in numbers in what RMHC and the paediatric healthcare system can do for families, together. For example, in Saskatchewan, RMHC Saskatchewan, Saskatchewan Health Authority and Victoria Hospital Foundation came together to introduce a new RMHC Family Room space in the NICU at Prince Albert Hospital, including 24/7 access to healthy, nutritious food for families, providing caregivers with essential rest and respite just steps away from bedside.
With the rate of inflation continuing to rise along with the cost of necessities like groceries – providing fresh and nutritious meals to families has never been more important. In fact, in 2022 RMHC across Canada served an impressive 300,000 meals – more than ever before.
“With a sick child, it’s not every day that we’re in the ideal state of mind to look after the kids perfectly. This place, and the meals – it takes care of everything.” – Ashmawy Family, 280 nights, RMHC BC & Yukon.
CATERING TO UNIQUE AND INDIVIDUAL NEEDS
Part of right-sizing the system also means acknowledging the unique needs of families as they navigate caring for a seriously ill child. 15% of RMHC families in Canada report at least one family member navigating a mental health challenge at the time of their stay at RMHC. More than a place to say, RMHC programming has evolved over the years to encompass the overall health and wellbeing of families – including music therapy, art therapy, and pet therapy. Dedicated spaces have also been created at Ronald McDonald House programs across the country to support mental health and wellness such as community gardens, wellness rooms, and meditation spaces.
With this evolution in programming, staff training has been at an alltime high over the past year. Mental
Health First Aid, Traits of an Inclusive Leader, The Construct of Race, and How to be an Ally are among the training sessions that have been conducted across the country to support and equip staff to better support families.
GROWING TO SUPPORT MORE FAMILIES
While RMHC across Canada is providing more support to families than ever before, the reality is that every 20 minutes, a family arrives at an RMHC doorstep, and we currently cannot meet the demand for our support. In fact, we estimate we’re meeting just 20% of the need for our House Program across Canada.
To ensure no family is turned away and every child can access the medical care they need, RMHC has ambitious plans to grow across the country, with a goal to double in size in the next 10 years from 554 to 947 bedrooms.

“As RMHC across Canada is only able to support 20% of the need today, growing our programming and number of bedrooms across the country is critical to ensure we can keep pace, continue to be there for more families who need us, and support our paediatric partners in en-
suring access to the healthcare families need,” says Kate Horton, CEO, RMHC Canada.
Most recently, this growth has come to life through RMHC Manitoba in 2022, which more than doubled its capacity from 14 to 40 bedrooms. This June, a new RMHC Family Room opened at CHU Ste. Justine in Montreal to support families within hospital walls. As we look to the near future, in 2024, a new House will open in Halifax, and the House in Ottawa will expand. In 2025, the House in Calgary will expand, and two new Houses will open in Prince Albert and Regina, Saskatchewan.
CONTINUING THE CONVERSATION
We look forward to continuing the conversation on how together, we can support the paediatric healthcare system on the journey to right-sizing across the country, at this year’s Children’s Healthcare Canada Annual Conference. Join our session on December 5 at 9:10 PT to hear what right-sizing means for primary care, mental health services, emergency care, surgery, research, community partners, and families with sick children. n H
SPONSORED CONTENT
To learn more about RMHC across Canada or to make a donation, visit: rmhc.ca.
AUGUST 2023 HOSPITAL NEWS 19 www.hospitalnews.com PAEDIATRICS
Ashmawy Family, 280 nights, RMHC BC & Yukon
Lochlin Baxter was diagnosed with Autism shortly before his third birthday. Autism therapist, Kiley Lortie, facilitates direct therapy sessions with Lochlin and his parents to de-sensitize him to foods without overwhelming him.
Autism program helps young patient build
healthy relationship with food
 By Kristen LoSchiavo
By Kristen LoSchiavo
M



cMaster Children’s Hospital (MCH) and Ron Joyce Children’s Health Centre (RJCHC) are home to one of the largest growing hospital-affiliated autism programs in Ontario. Services offered by the autism program at RJCHC include a clinical team which specializes in Applied Behaviour Analysis (ABA). ABA therapy focuses on building communication and daily living skills while reducing interfering or challenging behaviours. It can be provided in the clinic, at home, at school, and in the community.
As part of autism awareness we’re shining the spotlight on Lochlin, a young patient with autism who struggled to find food appealing. His ABA autism therapist, family, and healthcare team built a plan to develop and encourage healthy eating.
ABA THERAPY FOCUS
Lochlin Baxter was diagnosed with Autism Spectrum Disorder (ASD) at RJCHC shortly before his third birthday. His feeding behaviour had become a major concern and he wasn’t gaining weight. Following a case of stomach flu, his aversion to solid foods worsened, requiring hospital admission and the insertion of a gastrostomy tube (G-tube). A G-tube is inserted through the wall of the abdomen directly into the stomach. It is used to provide liquid and food to people who are unable to meet their caloric needs with oral feeding.
Now nine years old, Lochlin continues to use his G-tube but has been working with the staff at RJCHC to decrease his dependence on the tube, and to expand the amount and types of foods he will eat.


Autism therapist, Kiley Lortie, facilitates direct therapy sessions with Lochlin and his parents to de-sensitize him to foods without overwhelming him.
ACHIEVING NUTRITION GOALS


Lortie and the team had to be cautious when introducing new foods to Lochlin, making sure there were no problems with swallowing or choking.
“We started very small with Lochlin,” says Lortie. “We began with skills such as taking a lick of yogurt off a spoon and slowly worked our way up to expose him to larger amounts and different types of foods. Lochlin is such a fun, silly little guy and we were able to use that to find different ways of introducing food to make eating fun for him.”
Lortie also uses a reward-based initiative to help motivate Lochlin to eat meals and use positive coping skills. “He loves things like trivia and guessing games, so we have him take a certain amount of bites or finish a portion to earn clues or Google certain facts. It’s all about finding that middle ground and finding ways to keep him motivated.”
The team also worked at understanding why Lochlin struggled to accept new foods and helped him express his feelings about food in a positive way. Lochlin was extremely selective about the kind of foods he eats but by following the plan his health-care team developed, he has progressed very well with the program.
“Children with ASD can be turned off by food based on its texture, consistency, colour, or smell,”
Photos: Owen Thomas, Hamilton Health Sciences.
20 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com PAEDIATRICS
says Dr. Gillian Hogan, a pediatrician who works with Lochlin and Lortie. “It can take time to sort out why a child is struggling. For children who are fed by G-tube, progressing to oral feeding is often a lengthy process.”
COLLABORATING AS A TEAM
“If it wasn’t for Kiley and the team, there’s no way Lochlin would be where he is today,” says his mom, Amanda Baxter.
Lochlin has come a long way and can now take snacks to school and enjoy them with his friends.
Hogan, Lortie and Lochlin’s parents work together as a team to ensure his nutritional goals are being met. “Family is a huge part of the care team in our program,” says Lortie. “It’s great when everyone can come together and collaborate. It helps to create consistency and routine for the patient.”
Lochlin will sit with his family and eat meals together while using positive communication to express what foods he likes or dislikes. “Eating and using emotional coping skills are both hard things to work on, and he manages both very well,” says Lortie who has also joined Lochlin during family meals.

“Kiley’s awesome,” says Lochlin. “I always get so excited every time she comes over and we get to do things together like build Lego.”
ENCOURAGING INDEPENDENCE AND CHEERING-ON POSITIVITY
Lochlin loves to be independent, and as he progresses, he is open to more options and choices. “Asking what he wants to eat, which spoon he would like to use, and things like this help give him a sense of control that helps to build empowerment,” says Lortie.
Recreational opportunities offered at the RJCHC have helped to provide Lochlin with a positive community as well. For example, as part of the RJCHC cheer team he loves to promote encouraging messages like, “I can do this” and “I’ve got this” in his everyday life.
Moving forward, Lochlin’s healthcare team and family are continuing to gradually increase his food intake
orally while also boosting his independence and confidence.
“We should never put limits on where a child can go,” says Hogan. “Kids are resilient and Lochlin’s story is an example of pushing against those limits. I’m amazed at how far this young boy has come, and he’s grown so much since I’ve known him. It’s been a pleasure to work with him and his family.” n H
Shriners Children’s has been providing hope and healing to children for more than 100 years. Our compassionate, prestigious doctors and care teams are committed to excellence in care related to a number of different pediatric orthopedic conditions including muscular and neuromuscular conditions. Our individualized care plans can include physical therapy, occupational therapy, orthotics and prosthetics, care management and rehabilitation. Our services are available to children across the country as well as internationally.


Learn more at shrinerscanada.org
Kristen LoSchiavo works in communications at Hamilton Health Sciences.
AUGUST 2023 HOSPITAL NEWS 21 www.hospitalnews.com PAEDIATRICS
New extensive needs program wraps care around patient and his family
By Kristen LoSchiavo
For children with several medical, physical and developmental complexities and social vulnerabilities who need access to many different care providers, navigating the healthcare system can be overwhelming.
Hamilton Health Sciences’ McMaster Children’s Hospital (MCH) recently announced we are one of three Ontario hospitals that will collectively receive $97 million from the province over three years to launch a pilot program to help children and youth with complex special needs, along with their families. The program is jointly funded by the Ministry of Health and the Ministry of Children, Community, and Social Services.
The Extensive Needs Integrated Pathway program was developed to address the needs of children and youth with multiple diagnoses who require a team approach across physical, mental, behavioural, developmental health, and social vulnerabilities. While in the early stages, this program will be closely linked to existing services within MCH, as well as community agencies.
PUTTING YOUTH AND FAMILY FIRST
“Far too often, young people with extensive needs get lost in between existing programs and services,” says Bruce Squires, MCH president.
“We are creating a new model which puts these children, youth, and their families at the centre with expert medical, developmental, and social services wrapped around them. This unique collaboration between hospitals and our two ministry partners targets this significant need. McMaster Children’s Hospital is excited to move forward providing children and youth with this important care, allowing families to focus solely on their child’s well-being.”
Participating families will be connected to a team of professionals, including doctors, social workers and behavioural consultants who work together to provide tailored support

based on the individual needs of the child or youth, and their families.
One family that was recently introduced to the program says it has already started to help their child. They joined the program through MCH, receiving services out of HHS’ Ron Joyce Children’s Health Centre (RJCHC).
“Of course I jumped at the chance to be involved,” says the patient’s mother, who prefers that her family not be identified. “I was at my breaking point as I felt all doors were closing around me and my child, who was on waitlists and not seeing results. I struggled with many different obstacles, and my son was spiraling out of control due to his mental health issues, autism, ADHD, ODD (oppositional defiant disorder), and severe anxiety.”
The client and his family have been receiving support from his health-care team and have been connected to professionals who assist with his healthcare journey.
“Right from the start he was connected to a psychologist and an ABA (applied behaviour analysis) specialist,” says the patient’s mother. ABA therapy focuses on building communication and daily living skills while reducing interfering or challenging behaviours. “I immediately felt like things were changing for the better.”
School has been challenging but the program helped give a voice to the patient and his family. “I felt unheard as a parent,” says the patient’s mother. “I spoke to the team and was immediately contacted by another support system led by an ASD (autism spectrum disorder) consultant who works with my son’s school to provide the support he needs by attending meetings, providing feedback to the school, and working on plans for safety and his IEP (individualized education plan).”
Erica Siebert, an integrated service consultant on this patient’s team, recognizes the need to connect families to both hospital and community services.
“Navigating health and community systems and services can be extremely taxing on our families, especially families caring for children with extensive
needs,” she says. “Our role through the extensive needs program is to provide children, youth and their families with opportunities to feel empowered and supported while offering the right service at the right time.”
The patient’s mother says, “This program has helped my son gain confidence, regulate and control his outbursts, and he now participates in a PEERS Program set up by his healthcare team. I’ve always known that my child is creative, caring and can succeed in life, and this program and team are making this happen one step at a time.”
PARENT CHECK-INS
This program focuses on supporting families, ensuring all members involved with care have an outlet to access resources, and a space to look after their own physical and mental health needs.“Not only does my son get support but, as his parent, I also receive the support that I need as well,” says the mother. “The program has provided me with resources throughout this past year such as setting me up with a psychologist from the Family Check-Up program who helps me with
my everyday parenting skills and gives me confidence that as a parent I am doing the best that I can for not only my children but for myself.
The team has really taught me to take care of myself in order to be there for my children.”
Dr. Brittany Jamieson, a psychologist who works closely with this family, sees the value in having a team behind each family.
“The program’s team experience has allowed us to work effectively to reduce duplication in service, to provide consistent care and recommendations, and to bring together many perspectives and unique skillsets to address the family’s needs and concerns,” she says. “Families are doing the best they can and it is easier to do this with a united team supporting them.”
GIVING HOPE TO FAMILIES
Such support is vital to children and youth with extensive needs and opens doors for other families experiencing similar situations.
“We’ve seen so much change and progress throughout this journey.
Continued on page 24
From left to right: Dr. Rebecca Shine, Dr. Brittany Jamieson, Erica Siebert, Amanda Hendry, Dr. Irene Drmic, and Katrina Armstrong.
22 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com PAEDIATRICS
Photos courtesy of Hamilton Health Sciences
Lessons learned from shortage of children’s cold, flu medicine to create strong supply chain
 By Christine Donaldson
By Christine Donaldson
With cold and flu season still a few months away, HealthPRO Canada is building on lessons learned from last year’s critical shortage of children’s cold and flu medications to protect Canadian patients from a return of similar supply disruptions.
As Canada’s leader in healthcare procurement, we took immediate action when we learned of the imminent shortage of children’s cold and flu medications stemming from higher-than-expected cases of viruses, coupled with a surge in purchasing in community settings.
In partnership with Johnson & Johnson Australia, HealthPRO implemented a supply agreement to bring Tylenol™ for Babies to Canada which was made immediately available to over 1,300 healthcare facilities across the country and we facilitated supply to hospital pharmacies to lessen the burden on parents and caregivers in the community. In addition to helping bring in the foreign supply, we also entered into supply agreements with domestic suppliers to increase the availability of Canadian-labelled product to our hospitals.
The silver lining of being confronted by the crisis is that we are now better prepared to work with our health system partners to avert future shortages of critical medications for vulnerable populations like children.
Here are the top lessons we are building on from our work addressing last year’s shortage of children’s cold and flu medications:
NATIONAL REACH GIVES US POWER
HealthPRO Canada’s strong partnerships, national scope and global connections allow us to move quickly to find solutions – as we demonstrated through our ability to secure paediatric cold and flu medicine from international partners.
It’s also because of our national reach and expertise that HealthPRO Canada has been selected as the only hospital procurement agency to sit on a newly formed Health Products Supply Chain Advisory Committee created by Health Canada to further improve our ability to prevent and mitigate shortages.
INNOVATIVE PROCUREMENT PRACTICES STRENGTHEN OUR SUPPLY CHAIN
As part of our commitment to pursue world-class procurement practices, we are changing how we categorize and procure key paediatric medicines to better guard against shortages. We are looking at awarding multiple formats and more than one supplier for paediatric-specific products to create a more resilient supply chain for this vulnerable population of patients, a strat-
Christine Donaldson, President and CEO, HealthPRO Canada

egy we use across many other critical medication categories.
We are carrying on the torch from Health Canada in continuing a National Drug Reserve Program for vulnerable medications, such as sole source drugs, those with a history of shortages, and medications that don’t have alternatives. Our program will guarantee a pre-determined percentage of excess inventory for healthcare facilities to use during surge demand helping to avert interruptions in patient care.
PREPARATION IS KEY
We are developing a Healthcare Procurement Crisis Playbook to address future disaster planning including communications protocols and best procurement and contracting practices to mitigate the impacts of future disasters and supply chain disruptions, implementing best-in-class global practices.
EARLIER WARNING OF SUPPLY DISRUPTIONS IS NEEDED
HealthPRO Canada recognizes the power of data in driving informed decision-making. Our network provides us unique visibility and access to this critical information regionally and nationally across our Canadian supply.
We are taking action to drive insights from the data we collect to reduce the impact of drug shortages for all patients, including children. The best way to mitigate the impacts of disruptions that cannot be averted is for suppliers to provide early warning and accurate up-to-date information to us – this allows other partners in the chain to prepare proper contingency plans.
While it may not be possible to eliminate all supply disruptions, HealthPRO Canada is leading a stronger, more-resilient supply chain based on what we learned from working with our healthcare partners to navigate last year’s shortage of paediatric cold and flu medicine. n H
SPONSORED CONTENT AUGUST 2023 HOSPITAL NEWS 23 www.hospitalnews.com PAEDIATRICS
Mobile Public health dental program supports vulnerable youth
Keira Johnson remembers what it was like to be homeless and in pain.
“I was 16, living in a friends’ car, sleeping wherever I could, working full time and trying to finish high school,” says Keira. “My mouth was bleeding and I was in pain but I couldn’t afford to see a dentist.”
Fortunately, a youth support worker connected Keira to Fraser Health Public Health’s dental program for vulnerable youth, which operates out of the Mobile Health Clinic.
Helga Thordarson, a registered dental hygienist with Fraser Health, was able to assess Keira, work with a local dentist to come up with a treatment plan and find funding to cover the cost.
“For Keira it was 15, maybe 20 minutes in the van, and we did all of the behind the scenes work and phone calls to get her teeth fixed,” Helga says.
“I know we got her through a real rough patch in her life and a lot of our clients are going through rough times. Oral health may seem like a small thing but it has a big impact on people’s lives.”
The mobile dental program has helped more than 800 youth since it
Continued from page 22
launched in 2020. The clinic operates out of a van and primarily visits designated locations in Surrey with regular stops at Foundry in Langley.
In addition to dental care, the Mobile Health Clinic supports age 0-5 immunizations as well as sexual health/ blood borne diseases. All of the mo-
bile clinic’s services are designed to improve access to care for people who may face social barriers in receiving care from traditional sources.
“Being a kid and trying to figure out what am I going to eat, where am I going to sleep…in the scope of things, teeth may seem like a small thing but
the dental care made such a huge difference in my life,” Keira says.
“I graduated high school. I’m working and planning my career…my teeth, my life, it’s all good.”

The Mobile Health Clinic is a partnership between Fraser Health, Surrey Hospitals Foundation and TELUS. n H
Holland Bloorview Kids Rehabilitation Hospital in Toronto received new funding of $479,000 for its Get Up and Go (GUAG) persistent pediatric pain service – the first program of its kind in Canada. This brings total funding from Ontario’s Ministry of Health to nearly $1.3 million. The funding will help address increasing demand and higher complexity of mental health needs of the participants seen in the program.
“We are thrilled to receive this additional funding,” says A.J. Lopez, senior director, inpatient rehabilitation and complex continuing care (CCC) program. “The most challenging pediatric persistent pain cases in the country are seen by this team and many of them require enhanced care to address mental health needs. This additional funding will allow us to support families that need it the most.”
Extensive needs program
I’m more confident as a parent,” says the mother. “I’ve learned so much about autism and the challenges my son faces every day with all of his diagnoses. He’s worked very hard on himself and it brought us closer together as a family.”
“I feel that this program will help other children and their families by providing a support system that is unique to each individual and family situation,” says the mother. “It will provide resources that will help navigate their child’s needs, and give hope to families who are struggling with the challenges of raising a child with autism, as well as providing hope to the individual with special needs. I have
been lucky enough to participate in this amazing program, and I cannot say enough about how this program and my support team have made a difference in our lives.”
Siebert is pleased that the program has already made such a difference so soon after launching.
“The client and his caregiver continue to demonstrate resiliency and hard work as they engage with our team and the different services supporting them,” she says. “Seeing how a multidisciplinary team can come together and align their clinical goals while supporting and listening to their family’s needs demonstrates the need for this program.” n H
Specifically, the new funding will allow Holland Bloorview to:
• See more clients with increased complex mental health needs
• Improve quality of care for patients and families through enhanced intake coordination, reduced wait times and advanced data collection
• Increase access to GUAG’s multidisciplinary team of clinicians
• Increase staff support in the areas of intake, evaluation and research, physiotherapy, occupational therapy, social work and psychology

• Streamline referrals and admissions.
In addition, new staff resources will allow Holland Bloorview to better facilitate clients’ transition to community-based recreational opportunities, thus taking advantage of the functional gains they’ve made while
in the program. This has an additional impact of building community capacity to better support children and youth living with chronic pain in recreational activities.
“We are grateful to the dedicated team that runs Get Up and Go, and the transformational change we are able to make in the lives of young people experiencing chronic pain,” says Lori Palozzi, nurse practitioner and GUAG program lead. “Clients have shared their appreciation for the ‘constant support’ provided and the suggestion for future participants to ‘come in with an open mind.’ Families confirm that this program helps their child increase their function in a way that’s meaningful for them.”
Holland Bloorview’s GUAG program is Canada’s first inpatient multidisciplinary pediatric pain service that treats persistent pain (longer than three months) and supports children to regain function and return to usual activities like school and play. It consists of a two-week inpatient stay followed by a two-week day patient stay.
n H
Increased funding will help chronic pain management program address mental health
Kristen LoSchiavo works in communications at Hamilton Health Sciences.
Photo: Sam Polzin Photography
24 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com PAEDIATRICS
Get Up and Go multidisciplinary team members.





















WE ARE ON A MISSION TO RIGHT-SIZE CHILDREN'S HEALTH SYSTEMS Join us to transform healthcare systems for a growing population of kids in Canada. #WeCANforKids
Canada needs a paradigm shift to transform its long-term care Systems
Faced with a rapidly ageing population, staffing challenges and decades of funding shortfalls, longterm care systems in Canada require nothing less than a paradigm shift to remain viable into the future, a new report from the National Institute on Ageing (NIA) warns.
Enabling a More Promising Future for Long-Term Care in Canada is the third and final report in the NIA’s Future of Long-Term Care Policy Series. The first two reports, published in 2019, warned that if nothing changed, Canada’s long-term care (LTC) systems were on an untenable and unsustainable path. Since then, the COVID-19 pandemic has exposed and exacerbated many of the systemic issues plaguing the sector, such as workforce shortages and an over-reliance on institutional care when most Canadians would prefer to age at home. Families seeking LTC services today are faced with mounting costs, long waitlists, inconsistent quality levels, and the expectation that they will have to provide at least some unpaid care whether they can afford to or not.

However, Canada also has an opportunity to transform LTC to make it more sustainable, affordable and equitable. This report draws on what we have learned over the last three years of the COVID-19 pandemic, including expertise in financial and health policy, to create a feasible and fiscally responsible road map to ensure all older Canadians have access to high-quality LTC services.
“While the COVI9-19 pandemic shone a bright light on the cracks within Canada’s LTC systems, it has also spurred efforts toward system transformation,” said Dr. Samir Sinha, Director of Health Policy Research at the National Institute on Ageing. “It is critical to find and implement workable solutions quickly that will transform the organization, delivery and affordability of LTC services, while also
prioritizing the goal of enabling older Canadians to Age in the Right Place.”
The NIA’s proposed road map toward an improved LTC system includes four main components:
• Delivery of LTC services, with a focus on:
– Enabling integrated and holistic LTC that is primarily community-based, and institutional by exception;
– Enabling evidence-informed, person-centred care that is equitable, accessible and aims to meet not just needs but goals of care; and
– Enabling technologies to support Ageing in the Right Place.
• Workforce recruitment and retention, with a focus on enabling a LTC workforce that is appropriately supported and recognized.
• Affordability and sustainability, with a focus on enabling system sustainability and stewardship through more effective, efficient and sustainable financing arrangements.
• Data collection and monitoring, with a focus on enabling evidence-based decision making through data.
The pandemic’s lessons about health equity also underscore the importance of a person-centred approach to care that takes a broader look at care recipients’ circumstances and needs.
“A person-centred approach to LTC should be holistic, in order to appropriately understand and respond not only to people’s physical health, but also to consider mental health and social determinants of health,” said Dr. Ashley Flanagan, NIA Health Research and Policy Manager and lead author of the report. “It should consider the goals, circumstances and specific health and social needs of each person to provide them with more tailored and appropriate supports – which often results in better outcomes.”
KEY FACTS AND FIGURES:
• Within the next few years, Canada will join the ranks of other super-aged nations, with at least 21 per cent of our
population aged 65 years and older. By 2046, the population aged 85 years and older is projected to almost triple.
• In an NIA survey conducted in late 2020, 96 per cent of Canadians aged 65 years and older said that in light of the COVID-19 pandemic, they would do everything they can to avoid going into an LTC home.
• As of 2019, 64 per cent of Canada’s LTC expenditures were allocated to care in institutional settings such as nursing homes or LTC homes, and 18 per cent went to home and community-based care, compared to the more balanced OECD average of 52 per cent and 36 per cent, respectively.
• In 2019, Canadian households spent an additional $9.4 billion out of their own pockets to access LTC health services, on top of Canada’s governments spending $38 billion in providing LTC health services.
• In a 2015 national survey, 63 per cent of respondents said that their family was not in a good position, financially or otherwise, to care for older family members if they needed long-term health care and it worried them greatly.
• In 2021, more than 52,000 Canadians were on waiting lists for place-
ment in an LTC home, while about 167,000 Canadians aged 65 years and older were estimated to have unmet home care needs. Higher unmet care needs were reported in households in lower socioeconomic status areas.
• In the second quarter of 2022, the job vacancy rate for workers in LTC homes and retirement homes was 6.8 per cent, up more than threefold from 1.9 per cent in the second quarter of 2015. For all industries, the job vacancy rate grew to 5.9 per cent from 2.9 per cent in the same period.
• The number of Canadians who will need the support of unpaid caregivers is projected to increase from 345,000 to 770,000 by 2050, an increase of 120 per cent; however, due to declining birth rates, there will be 30 per cent fewer family members and friends to provide unpaid care in 2050 than there are today.
• Approximately 35 per cent of working Canadians balance paid work with unpaid caregiving duties; as of 2020, one-third of unpaid caregivers reported experiencing distress, up from 16 per cent in 2010. n H
26 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com LONG-TERM CARE NEWS
This article was submitted by the National Institute on Ageing, a think tank at Toronto Metropolitan University (formerly Ryerson University) focused on the realities of Canada’s ageing population.
Discovery could unlock new treatments for MS, Alzheimer’s disease
By Marlene Leung
AUnity Health scientist has revealed a new cellular interaction that aids in the regeneration of damaged myelin, the protective layer that coats nerve cells in the central nervous system. The discovery could lead to the development of new drug treatments for Multiple Sclerosis and other neurodegenerative diseases, including Alzheimer’s disease, she says.
The discovery, recently published in the science journal Nature Communications and chosen as an Editor’s Pick, was led by Dr. Veronique Miron, scientist at the Keenan Research Centre for Biomedical Science and John David Eaton Chair in MS research at the BARLO MS Centre.
Miron’s research lab focuses on identifying new treatment strategies
for neurological conditions where myelin is damaged.

“MS is a condition that primarily impacts people in the prime of their lives, and Canada has one of the highest rates of MS in the world,” she said. “I’ve always wanted to have a positive impact on patients with this condition through research.”
The surprising role of astrocytes
Miron and her lab discovered that star-shaped cells in the central nervous system called astrocytes play a critical role in repairing myelin. Myelin, a protective layer of protein and fats that wraps around nerve cells, is important because it allows our nerve cells to quickly send and receive electrical signals that control every aspect of our body’s functioning.
Cells in our brain called oligodendrocytes make and repair myelin. But certain diseases and conditions, such
as MS, cause oligodendrocytes to die and in turn lead to damage to myelin, slowing down the transmission of our body’s electrical signals. This is what causes the symptoms of MS, which can include loss of vision, loss of function in an arm or leg, spasms and difficulty walking.
Miron’s research team discovered that astrocytes help keep oligodendrocytes alive by supplying them with cholesterol.
The team examined brain tissue from people who had MS, and observed that in lesions where myelin repair had failed, the astrocytes were not making as much cholesterol compared to lesions where myelin repair was occurring. Importantly, in an experimental model, the team discovered they could improve myelin repair by boosting the cholesterol-giving properties of astrocytes with drugs.
“We find this study really exciting because we’ve discovered that astrocytes play a critical role in myelin repair, the pathway they use to lead to this repair of damaged myelin, and also drugs that we may be able to use to target and boost this pathway,” Miron said.
The research team believes the findings will also be important in developing treatments for ageing and Alzheimer’s, where myelin is also damaged.
“We’ve moved along quickly with this one study, and we’re hoping to continue with that kind of acceleration as we work to understand how we can use these drugs to treat MS patients,” Miron said, noting that currently there are no approved treatments aimed at enhancing myelin repair.
“We are working as quickly as we can to translate these findings into meaningful treatments for people with MS.” n H
What is home care?

Home care is about trust. It is feeling comfortable with a provider coming into the home of someone you care for and, possibly, assisting with the most intimate care.


Bayshore’s home care services are extensive, varied, and personalized for each individual. Whether it’s just a little assistance for daily tasks or round-the-clock care, Bayshore’s caregivers can help your loved ones to live their best life while remaining at home.
1.877.289.3997
talk.
Let’s
PERSONAL CARE | HOME SUPPORT | NURSING
bayshore.ca
AUGUST 2023 HOSPITAL NEWS 27 www.hospitalnews.com LONG-TERM CARE NEWS
Marlene Leung works in communications at Unity Health.
My social work background serves me well as hospital CEO
 By Jorge VanSlyke
By Jorge VanSlyke
Ididn’t realize the extent of my privilege until I looked back and traced my journey from being a social worker in the Philippines to my current role as President and Chief Executive Officer of Blanche River Health, a two-site hospital in Kirkland Lake and Englehart, located in Northeastern Ontario.
Social Work was not a popular nor known profession in the Philippines back in the 90s. The stereotypical association was philanthropic in nature, with many expressing bewilderment that there was a whole degree associated with giving relief goods. I knew firsthand because those were the comments thrown my way after family and friends learned of my degree of choice. It was not my primary choice, but it was one of the few remaining programs available if I wanted to get a scholarship.

What came as a surprise was the deep appreciation of the learnings throughout the program. In a developing country context, social work’s curriculum was centered on individuals, groups, and communities, highlighting the person in environment concept, conflict management, group facilitation and community development.
Community development was a strong core program due to the realities of urban poverty and rural underdevelopment. Resources were scarce so our training was in leveraging the system and the communities as our primary clientele when providing services instead of individuals. This was not the same focus when I moved to Canada and completed my Master of Social Work. In a developed country context, I found the core programs to be highly individualistic with a strong focus on an anti-oppressive lens and advanced clinical practice skills.
Aside from earning two post-secondary degrees in Social Work in two different countries, I also practiced the profession as a frontline Social Worker for five years before switching to management.
As I reflect back, I was amazed at how much my fundamental leadership precepts benefited from what I learned in Social Work:
PERSON IN ENVIRONMENT AND SYSTEMS THINKING
An individual cannot and should not be viewed as a separated, isolated entity from his/her system. To understand the individual is to understand the history, interconnections, and the social and physical environment. As a leader, this training helped me evaluate problems within the context of intricate and interrelated systems. It helped me understand that there is no such thing as quick fixes. It helped me view problems and situations within their context and aimed for sustainable solutions by leveraging the resources available and encouraging out of the box thinking.
ANTI-OPPRESSIVE FRAMEWORK AND CRITICAL THINKING
Learning the anti-oppressive framework helped me unpack my own biases and prejudices. This was a pivotal learning as it sharpened my understanding of self as it relates to others. As a hospital CEO, being aware of the power that I hold in my position was just one part of the equation. I learned to continuously reflect on my own thought processes and the rationale behind reactions and decisions. I also learned to view individuals and situations within context, seeking to understand first, and having a broader understanding on where an individual may be coming from. This skill set is deeply embedded in my own leadership practice as I pursue truth and justice in my everyday world.
CONFLICT MANAGEMENT AND GROUP DYNAMICS
Learning to view individuals within their context allows me to look behind
the person’s presentation and drill down to the core issue behind a complaint, a feedback, and a situation. My professional training helped me regulate and set aside my emotional reactions and focus on where the person in front of me is coming from. This is a key skill set in conflict management and resolution. I remember learning various techniques in de-escalating situations and in facilitating conversations, including understanding the verbal, non-verbal, and paraverbal cues around me. I adjust my communication styles accordingly. These skills continue to serve me well as a leader especially since leadership is predominantly centered on managing relationships.
PURPOSEFUL SHARING OF SELF
One of Social Work’s core principles is the purposeful sharing of self as part of the therapeutic process. In
a leadership context, sharing personal vulnerability, sharing snippets of my history and context, with clear and intentional purpose in mind, allowed people around me to be vulnerable as well and to see me as a person occupying a role. This helped me engage with people in meaningful ways and is the basis of my collaborative persona.
Social Work as a profession is all about people. It is a “helping” profession but it goes beyond individual needs. It recognizes the role of groups, communities, and systems as a whole and it trains you to be a facilitator of sustainable changes. And as a leader in healthcare, with all the complexities that we face in our day to day world, I feel fully equipped to navigate my world because of who I was trained to be.
Going back in time, Social Work was not only my primary choice, but my only choice. n H
Jorge VanSlyke is President and CEO of Blanche River Health, a Northeastern Ontario hospital with two sites.
28 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com FROM THE CEO’S DESK
Jorge VanSlyke is President and CEO of Blanche River Health
Offload Specialists bridging the gap between pre-hospital and hospital care
As part of an innovative new initiative to help reduce ambulance offload delays, provide hands-on support to frontline healthcare workers, and enhance access to care, Cornwall Community Hospital (CCH) has hired three paramedics who will serve as new Offload Specialists in the Emergency Department.

Offload Specialists will play a vital role in supporting paramedics during the offload process at the hospital’s Emergency Department. Often paramedics experience delays in transferring lower urgency patients to the Emergency Department due to the high demand on hospital resources. By introducing Offload Specialists, CCH aims to streamline this process, ensuring a seamless transition for patients while allowing municipal paramedics to return to the field more promptly.
Their responsibilities will also include working in collaboration with
the care team to provide patient care within their scope of paramedicine practice and standards, gathering necessary patient information, coordinating with hospital personnel, ensuring a safe and comfortable environment
for patients, and assisting with any required tasks.
“We are proud to introduce these new Offload Specialist positions at Cornwall Hospital as part of our ongoing efforts to enhance access to care,”
OCTOBER
said Jeanette Despatie, President and Chief Executive Officer at Cornwall Hospital. “We believe this new role will have a significant impact on our emergency services and will strengthen the entire continuum of care for our community.”
“The creation of the Offload Specialist positions is a testament to our hospital’s commitment to collaboration and innovation in healthcare delivery,” said Dr. Anastasios Boubalos, Chief of Staff at Cornwall Hospital. “These new Offload Specialists will not only enhance patient care and safety at CCH, but also enable our local paramedics to focus on what they do best – saving lives.”
Successful applicants were hired earlier in July and are currently undergoing hospital orientation and training to ensure they are equipped and prepared to provide exceptional care within the hospital environment. n H
SEPTEMBER FOCUS: Emergency Services/Critical Care/ Trauma/Emergency/Online Education: Innovations in emergency and trauma delivery systems. Emergency preparedness issues facing hospitals and how they are addressing them. Advances in critical care medicine.




OCTOBER FOCUS: Mental Health and Addiction/ Patient Safety/Research/Infection Control: New treatment approaches to mental health and addiction. Developments in patient-safety practices. An overview of current research initiatives. Developments in the prevention and treatment of drug-resistant bacteria and control of infectious (rare) diseases. Programs implemented to reduce hospital acquired infections (HAIs).
Advertising Booking Deadline August 25th
Material Deadline August 29th

For more info email advertising@hospitalnews.com
Advertising Booking Deadline September 22nd Material Deadline September 26th
For more info email advertising@hospitalnews.com
NOVEMBER FOCUS: Technology and Innovation in Healthcare /Artificial Intelligence (AI) /Patient Experience/ Health Promotion: New treatment approaches to mental health and addiction. An overview of current research initiatives Programs and initiatives focused on enhancing the patient experience and family centred care. Programs designed to promote wellness and prevent disease including public health initiatives, screening and hospital initiatives. Annual Medtech Supplment.
Advertising Booking Deadline October 20th
Material Deadline October 24th
For more info email advertising@hospitalnews.com
From left: CCH Offload Specialist Sophie Tasse, Cornwall SDG Paramedic Calla Legue, and CCH Offload Specialist Lee Montford in the Ambulance Bay at Cornwall Hospital.
UPCOMING EDITIONS NOVEMBER
SEPTEMBER
AUGUST 2023 HOSPITAL NEWS 29 www.hospitalnews.com NEWS
Ensuring our patients’ “Voyce” is heard
By Ellie Stutsman
Accessing Canada’s healthcare system can be a frightening and stressful experience for those with a language barrier. For patients and their families who are not proficient in English, they may struggle to express their concerns and symptoms and to understand medical terminology. This can lead to misunderstandings, frustration and even a lack of trust between patients and health-care providers.
“People are at their most vulnerable state when trying to access health
services, and the inability to speak in their native tongue to clinicians is an incredibly challenging barrier,” says Ted Scott, chief innovation officer at Hamilton Health Sciences (HHS).
“So, we’re excited that Voyce can help us overcome this barrier and create a more seamless experience when accessing health care in our community.”
A COMMUNICATION SOLUTION
As one of Ontario’s largest and most comprehensive health-care organiza-

tions, HHS recognizes the importance of equity, diversity, and inclusion in delivering exceptional care to our diverse community of 2.3 million people.
When it comes to interpretive services, HHS previously relied on in-person interpreters or phone services, however, they were time-consuming and often unavailable in a timely manner.

“Improving communication is essential to us as an organization that’s on a mission to provide ‘best care for all,’ says Scott. “Voyce was identified as an opportunity to serve our commu-

nity better, but we needed to evaluate it in our organization to understand where and how we could best use this service.”
Ontario Bioscience Innovation Organization (OBIO®), a not-for-profit organization dedicated to advancing health technology innovation and commercialization, facilitated a partnership between HHS and Voyce Canada. This Toronto-based technology-driven company offers a language interpretation solution. Through this partnership, HHS is evaluating
A ‘black box’ to assess and train expert surgical teams
Just like the airline industry has a black box to learn from, hospitals can now use recordings taken during surgical procedures to help train expert surgical teams.
Developed and commercialized by a team at St. Michael’s Hospital, Sunnybrook researchers are bringing a black box-like technology into the world of assessment – using it for the first time to evaluate performance and direct the training of expert
teams in an operating room (OR) setting.
“If you measure something, you can improve it,” says Dr. Markku Nousiainen, orthopaedic surgeon at Sunnybrook Health Sciences Centre. “Our goal is to measure individual and team performance in the OR and use that information to develop teaching tools to improve performance with the goal to improve patient outcomes.”
This initiative focuses on patients having surgery to repair a hip fracture,
as these patients can experience variations in outcomes. Research has shown that patient outcomes after surgery depend on more than just the performance of the surgeon – outcomes also depend on the entire surgical team including nurses, anesthesiologists, radiation technologists, and trainees.
“In order to optimize patient outcomes, we must ensure that the entire OR team performs at the highest level of expertise,” says Dr. Cari Whyne, research director of Sunnybrook’s Holland Bone and Joint Program, and a professor at University of Toronto.
“However, we need to understand more about what expertise for a surgical team looks like, so that we can develop teams that perform at this level. This will help us minimize the current variation in surgical quality.”
The Sunnybrook pilot project will record videos and dialogue within the operating room, helping researchers measure skill levels and collaboration between team members. This information will be collected during hip fracture surgeries and analyzed to determine which aspects of surgical team performance and workflow can be improved, and to identify connections to patient outcomes.
“The continuous monitoring of the surgical environment and analyt-




ics will provide us with an objective data set to look at, allowing us to evaluate how the team members are performing without having to rely on individual recollections,” says Dr. Nousiainen, an associate professor at the University of Toronto. “Remembering is subjective and is subject to bias.”
Not actually a ‘black box’, the black-box-like technology uses small cameras installed around the OR and buried inside the overhead surgical lights. The equipment records audio, multi-resolution video, patient vitals and intraoperative x-ray imaging. The data is collected onto privacy-safe software and securely transferred to analysts to assess performance. A twin system has also been installed in a non-clinical OR for the purposes of training.
Sunnybrook’s leading team of orthopaedic specialists will determine how to provide expert, team-based surgical training and care in the operative management of hip fractures. “Our anticipated results will help establish best practices for delivering expert care to all orthopaedic patients,” adds Dr. Whyne.
The project is supported by a $3 million investment by the Wyss Medical Foundation. n H
important
ParaMed Home Health Care www paramed com/careers Registered Nurse Our team goes wherever our patients need them, ensuring they can remain in their own homes safely and comfortably Join our team of Nurses, HSW's PSW's
Everything I do has such an
impact.”
v Susan
30 HOSPITAL NEWS AUGUST 2023 www.hospitalnews.com NEWS
Voyce’s medical interpretation platform.
To access Voyce, patients and their care team simply need an internet connection and a device such as a smartphone or tablet. There is a diverse network of 2,000+ qualified interpreters in more than 240 languages who are trained in medical terminology, with an average connection time of less than 30 seconds.

REMOVING THE LANGUAGE BARRIER
Voyce has been deployed at HHS in select units representing a variety of settings including an emergency department, inpatient and outpatient units. This allows any adoption barriers to be assessed before full implementation is considered not only within HHS but across any other health-care organization.
“Having the Voyce translation service really helps to promote allyship and inclusivity for a lot of our families who don’t speak English,” says Dr.
Audry Lim, Pediatrician and Medical Lead of Complex Care at HHS McMaster Children’s Hospital (MCH).
“Without the ability to interpret properly and timely, I find that it really impedes the care we can provide. But, by pulling Voyce into the room I can communicate with the families in real-time without any translation issues. It really helps to reassure the family and answer their questions immediately.”
By providing real-time interpretation services, care teams can ensure that patients and families can fully understand their medical conditions, treatment options, and instructions for follow-up care.

Aisha and Mahmoud Jomaa’s daughter Aline is a patient at MCH with multiple specialists including Dr. Lim. They have been able to utilize Voyce since the pilot began.
“I know that with Aline’s condition, we need to come to the hospital a lot, so it’s very comfortable for me to have this service,” says Aisha. “Whatever I’m saying, I’m sure that it’s being re-
layed, no matter how I’m expressing it, in the same way. It feels like I’m the one who is speaking.”
VOYCE FOR ALL
Patients, staff and physicians have had extremely positive feedback on Voyce, so HHS has currently extended the pilot while it works on securing it
as a standard service that can be accessed organization-wide.
“We’re also going to extend the service into our research and education areas as well, to help us better understand the needs of our non-English speaking community,” says Scott. He continues to say, “Voyce is game-changing.” n H
Ellie Stutsman works in communications at Hamilton Health Sciences.
Aisha and Mahmoud Jomaa with their daughter Aline, and Hamilton Health Sciences nurse practitioner Maddison Gilmour.
AUGUST 2023 HOSPITAL NEWS 31 www.hospitalnews.com NEWS
Photo: Josh Carey, Hamilton Health Sciences







